|
Wisdom Teeth Removal Complications
What are the risks of an operation to remove impacted wisdom teeth?
The information presented on this site is of personal opinion and consequently is slanted and biased and not based on proper scientific research. The information presented is NOT written by a dental expert. Further the information presented has NOT been subjected to peer review by experts to verify accuracy and data integrity.
All operations have risks, and the surgeon performing the surgery should discuss some things that could go wrong. It is important to remember that the standard of care (in the U.S.) is not to go through all of the possible side effects and complications that can occur.
Some of these complications below are common whereas others are quite rare and some dentists and oral surgeons may not even know they have occured after wisdom teeth removal. The incidence or amount of time one would expect a complication to occur is not well known for many of these complications. Do not be misled to believe that all of these complications can occur with any sort of equal probability. A few of these complications occur much more frequently than others.
It’s hard to say exactly how often problems happen with surgery to remove wisdom teeth. About 1 in 10 people get problems during or after an operation to take out their wisdom teeth. These problems aren’t always serious or permanent. More serious problems may occur for those older than 25 and/or have deeply impacted wisdom teeth.
If you are looking to minimize risks please discuss your medical history with your physician, dentist, and surgeon and postpone (as in delay) any potential scheduled extraction(s) if you have any severe upper respiratory symptoms such as cough and cold. You may also consider 3-D cone imaging.
This page is not for for the faint of heart so please do not read any further. No discussion below is made of those who have succesfully had any wisdom tooth extracted with no complications and problems. Many complications that can potentially occur are the result of unfortunate mistakes without intent to harm. In very rare instances deliberate intentional harm can occur which is not a complication but still an unfortunate risk and discussed below.
If you have a problematic wisdom tooth or wisdom teeth you should seek medical treatment and NOT continue reading.
Millions of people have succesfully had wisdom teeth removed without problems. Many of the complications below are highly unusual and extremely rare. In addition a few of the case descriptions described did not occur in the U.S. Further some of the complications occured many many years ago and would clearly not be representative of the care one would reasonably expect to receive today.
Now without further ado here are the wisdom teeth removal complications:
1. Swelling, Discoloration, Pain, Malaise, Bruising, and/or Discomfort
It is of course possible to develop soreness, pain, malaise (feeling out of it), swelling (edema), discoloration, and/or discomfort after wisdom teeth removal. This can occur at the post extraction socket, any injection sites, in your face, and/or jaws which would require you to take it easy and rest at home for several days. Swelling caused by teeth removal is quite normal and usually will reach its maximum 48 to 72 hours after surgery. Swelling occuring more than three days after surgery may indicate infection. Pain, swelling, trismus and general malaise occur in about 50% of all patients who have a wisdom tooth extracted within the first few days. Discoloration of your face may appear black and blue and then change to a yellowish color after a few days. [105, 122, 153]
If any intravenous medication was used inflammation, stiffness, bruising (ecchymosis), and/or soreness could develop along the vein which may temporarily limit the full use of the arm where the injection occured. In rare instances this could cause long term discomfort and/or disability. [122]
2. Disruption to Your Regular Schedule and Activities
You may need to miss work or school for a few days and also not follow your normal daily living routine. After wisdom teeth removal people take off work/school an average of 1.26 to 3 days with a range from 0 to 10 days. You may also have some difficulty chewing and speaking as you normally would. [74, 75, 105]
3. Bleeding
Everyone bleeds after surgery, but it should stop completely within six hours after surgery. Less than 1 in 100 people have persistent or excessive bleeding that is difficult to stop. If bleeding is increasing after six hours after surgery you should seek medical treatment. Small amounts of blood within the first 48 hours after extraction is normal. Biting down on gauze or using your hand to apply pressure to gauze can help stop bleeding. Using a moistened tea bag and applying pressure to it can also help if gauze is not successful. Tea contains tannins which are plant polyphnols which can help stop bleeding. It is also possible to have a slight bleed from the nose for a day or two. [153]
4. Difficulty Opening Mouth (Trismus)
It is possible to develop trismus which means not being able to open your mouth as wide as you could previously. Your jaw could become locked and feel stiff and you could have difficulty eating food normally, talking, and/or brushing your teeth. This could be because of injury of the medial pterygoid muscle caused by a needle, your mouth was stretched open for a long time during surgery, inflammation, hematoma, and/or swelling. This is usually temporary. [31, 101. 122]
5. Dry Socket (Alveolar Osteitis)
Dry socket is when a throbbing pain occurs after removing a wisdom tooth when a blood clot does not form properly in the socket. When a blood clot is not present the jaw bone and pain receptors in the jaw bone are completely exposed.
The extraction site will become irritated and pain occurs due to the bone lining the tooth socket becoming inflamed. The symptoms are made worse when food debris trap in the tooth socket. A dry socket presents as a sharp and sudden increase in pain which usually starts around 3 to 5 days after a wisdom tooth extraction. It may start at night and you may first notice a dull throbbing ache in your ear which radiates towards your chin.
Dry socket likely occurs between 5% and 30% of the time after a wisdom tooth extraction as reported by most studies. [107, 170]
Dry sockets can heal in a couple of weeks without treatment. Dry socket is not an infection and is inflammation within the bony lining of an empty tooth socket. [108]
To prevent dry sockets you should avoid the following for atleast 3 days after having a wisdom tooth extracted and following the instructions provided by the surgeon:
- Smoking, spitting, vigorous rinsing/swishing with water, and/or suction (drinking with a straw)
- Activities that change the pressure inside of the mouth, such as playing a musical instrument
- Exercise (any vigorous physical activity)
- Coughing and sneezing
- Drinking carbonated beverages (such as pop, soda, and/or alcohol)
It is suggest for women to schedule any wisdom teeth extractions during their menstrual cycle to decrease their risk of developing a dry socket. [170]
Learn more about dry socket tips, advice, and information. [118]
6. Reaction to Medications (such as Anaphylaxis and Angioedema)
Anaesthetics and other medications provided during oral surgery can have side effects. You may need to not eat and not drink anything for at least 6 to 8 hours prior to surgery depending on the type of medications you are given. If you are given certain medications when you have recently eaten you could vomit and throw up which could become life threatening. [98]
You could experience drowsiness, nausea, and/or vomitting from the medications provided. In addition medications could cause itching, rashes, and/or hives.
You could experience an allergic reaction due to anesthesia or another chemical given known as anaphylaxis. This can result in widening of the blood vessels (vasodilation) which can lead to a sudden fall in blood pressure. Breathing or heart problems can subsequently occur. [64]
Many of the known risks and complications from anesthesia include airway blockage (bronchoconstriction), laryngospasm, asthmatic attack (bronchospasm), respiratory arrest, hypoventilation (respiratory depression), hypoxia (lack of oxygen), hypercarbia (too much carbon dioxide), cardiac arrest, cardiac arrhythmia, angina (chest pain), myocardial infarction (heart attack), syncope (fainting), seizure, stroke, malignant hyperthermia, pulmonary edema (fluid accumulation in the lungs), organ damage, ocular (eye) injury, phlebitis (inflammation of a vein), and peripheral or central neurolgic deficit. These problems are serious. If you have any allergies and/or asthma, you must tell your doctor. [64, 72, 96]
You could also experience a reaction to a medication provided known as angioedema. Angioedema is rapid swelling of tissues and could lead to an anaphylactic reaction or a life-threatening airway blockage if swelling was to occur in the throat.
If you are female and on birth control pills, medications given could neutralize the effects and allow for pregnancy to occur (this includes antibiotics). [53]
I encourage you to learn more about the differences between anaesthesia and sedation as you have a choice/input in the medications provided if you elect to have any of your wisdom teeth removed.
A healthy 17 year old had 4 impacted wisdom teeth removed under general anesthesia. She suffered a grand mal seizure and was transfered to a hospital and continued to have seizures every hour. Later the patient was released. [106]
See the Death section below for descriptions of cases where people had asthmatic reactions while under anesthesia to remove their wisdom teeth and died.
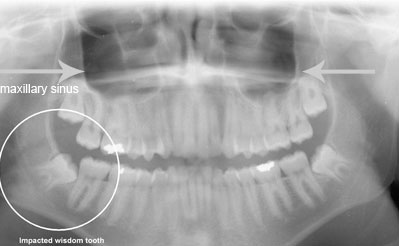
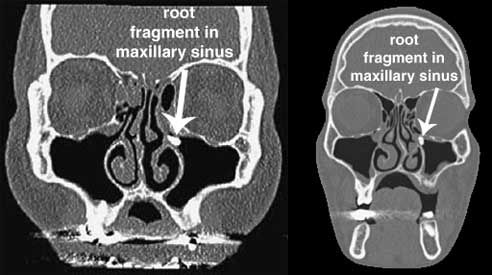
7. Mouth-Sinus Hole (Oroantral Communication)
The upper wisdom teeth roots are very close to the maxillary sinus and some people even have roots that go into the sinus. An opening into the sinus after the removal of wisdom teeth occurs once in a while which is known as a mouth sinus-hole or an oral-antral communication. If this occurs it is likely that bacteria can prevent healing and get into the sinus. The infection that results is called sinusitis which does not respond well to antibiotics and may require additional surgery in order to drain the sinus.
With a mouth-sinus hole, a material called gelfoam is typically placed in the extraction site to promote clotting and serve as a framework for granulation tissue to accumulate. If this does occur patients are often given antibiotics, decongestants, should avoid certain activities, and should see an Ear, Nose, and Throat (ENT) Doctor.
Sinusitus can potentially lead to numerous complications, some of which are deadly and require immediate surgery. Sinusitus complications include brain abscess, meningitis, orbital abscess, orbital cellulitis, epidural abscess, subdural empyema, cavernous sinus thrombosis, and osteomyeltis all of which are known to have occurred after wisdom teeth removal and described in greater detail below. In addition, sinusitus can lead to nasal polyps and mucoceles. Nasal polpys can lead to difficulty breathing and potential permanent loss of smell. Sinus mucoceles, if infected with bacteria, can become life threatening. [48, 49]
A man in his late 20's had a partially erupted upper right wisdom tooth that was bothering him. His oral surgeon decided to also remove the upper and lower left impacted wisdom teeth that were causing no problems even though the upper left wisdom tooth was close to the maxillary sinus wall. The man complained of subsequent pain and swelling below his left eye and along the checkbone, a high fever, malaise (feeling out of it), and bad smelling nasal discharge. The oral surgeon was somehow led to believe the man had a dry socket which he treated and later said the man didn't need any more treatment. Around a month after the extractions the man felt dizzy and disoriented and was brought to an emergency room. His left maxillary sinus was found to be completely filled with fluid and he had emergency surgery performed. He later had subsequent sinus surgeries. Many years have passed and he continues to have severe and debilitating sinus headaches and paroxysms of shooting pains in his head and jaws which likely will occur for the rest of his life. This case is described by Jay W. Friedman in his excellent book titled Complete Guide to Dental Health . [140] . [140]
A 31 year old male had all 4 wisdom teeth removed and developed a headache 2 weeks after surgery. His dentist told him that his sinus cavity had been penetrated during surgery. He was prescribed pain relievers and antibiotics which were not effective. He responded to a survery on teethremoval.com and says he continues to have severe headaches everyday and at the time of his survery response it had been 3 months since his wisdom teeth were extracted.
Unfortunately, a finding of sinusitus after having an upper wisdom tooth extracted can pose a potential dilemma.
8. Oroantral Fistula
The communication between the oral cavity and maxillary sinus (oraantral communication as described above) can becomed lined with epithelium (skin) and lead to the development of an oroantral fistula. The fistula causes the sinus to be permantely open which allows for the passage of bacteria from the oral cavity into the maxillary sinus which can lead to inflammation. The orantral fistula has the possibility of becoming chronic and needs to be closed quickly. An oraantral fistual has a reported incidence of 0.008% to 0.25%. The orantral fistula will likely need to be closed surgically for larger fistulae using a buccal advancement flap or palatal island flap. For smaller fistulae surgery may not be needed. [35, 82, 100, 105, 143]
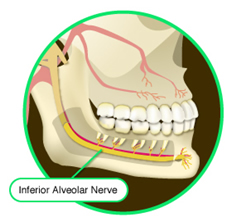
9. Nerve Damage
Nerves in your mouth may be damaged during surgery to remove your lower wisdom teeth. Your lip, chin, check, teeth, and/or tongue may feel tingly, tickly, or numb (paresthesia).
The branch of the trigeminal nerve, called the mandibular nerve, and it's branches are the nerves most likely to be damaged during wisdom teeth removal. The 2 most common nerve's damaged are the lingual nerve and the inferior alveolar nerve. In some cases the nerve damage is temporary and the nerve heals itself where as in other cases the nerve is left permanently damaged.
The lingual nerve is the nerve that helps you sense pain and temperature in your mouth. If it is damaged it could affect your ability to taste. Dentists and surgeons often use an instrument called a lingual nerve retractor to move the nerve out of the way during surgery. But this can actually increase the risk of damage. If the lingual nerve is damaged it could cause tingling, tickling, or numbness of half the lower lip and chin on the affected side.
The reported incidence of lingual nerve damage is 0.1% to 22%. This means that up to 22 out of 100 people having their wisdom teeth removed could have lingual nerve damage. However, it is important to keep in mind that these studies look at a sample of the whole population. Hence, the reported number could be much higher than it actually is for the true average of everyone who has their wisdom teeth removed. The upper percentage of lingual nerve damage may be closer to 2%. [4, 15, 105, 167]
The inferior alveolar nerve supplies sensation to the lower teeth on the right or left half of the dental arch and the sense of touch to the right or left half of the chin and lower lip. If the inferior alveolar nerve is damaged it could cause tingling, tickling, or numbness on a side of the tongue.
The reported incidence of inferior alveolar nerve damage is roughly 0.5% to 5%. This means that up to 5 out of 100 people having their wisdom teeth removed could have inferior alveolar nerve damage. [15, 105, 167]
One recent study reported that if the lingual or inferior alveolvar nerve was damaged during surgery than over 50% of the time after 6 months the nerve had completely healed. This means that those not in the included percentage were left with lasting nerve damage which in a few cases continued to heal but in others became permanent. Based on studies, a good measure is that for less than 1 in 1,000 people after wisdom teeth removal, the numbness caused by nerve damage is permanent, whereas others will regain feeling. If a damaged nerve has not healed within 12 months the damage is usually permanent. [1, 15, 74, 105, 167] However, cases have been reported of recovery after 12 months of damage. [171]
Other nerves can be damaged as well so I encourage you to learn about nerve damage more in depth! See the dental malpractice page for numerous case reports of nerve damage occuring after wisdom teeth removal.
The risks factors for inferior alveolar nerve damage when removing the lower wisdom teeth are increasing age, unerupted wisdom tooth, deep impaction, intra-operative inferior alveolar nerve exposure, and the surgeon using the lingual split technique. The risk factors for lingual nerve damage when removing the lower wisdom teeth are increasing age, unerupted wisdom tooth, distal impaction, the surgeon raising the lingual flap, and the surgeon using the lingual split technique. [110] Horizontal and mesioangular impacted wisdom teeth may result in more nerve injuries. [143]

10. Maxillary Tuberosity Fracture
An upper (maxillary) wisdom tooth is directly in front of the maxillary tuberosity. Thus a maxillary tuberosity refers to the hump which is behind one of your two upper back teeth on both sides which have gum tissue covering the underlying bone. It is possible that when an upper wisdom tooth is extracted some of the bony socket can come out as well and thus the maxillary tuberosisty can be fractured. A maxillary tuberosisty fracture may occur in 0.6% of all wisdom tooth extractions. This typically requires a splint for 4-6 weeks. A maxillary tuberosity fracture could potentially cause a mouth-sinus communiction (ora-antral communication). [32, 105, 122]
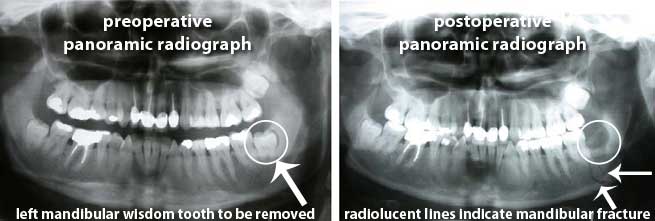
11. Lower Jaw Fracture (Mandibular Fracture)
The lower jaw can be fractured during or after removing a lower wisdom tooth. This is known as a mandibular fracture. It is important to note that a mandibular fracture can occur during surgery (immediate mandibular fracture) or it can occur sometime after surgery (late mandibular fracture) which is usually within the first 4 weeks. [33, 57]
An immediate mandibular fracture can occur with excessive force to the lower jaw and improper instrumentation by the surgeon. [33] Small forces can also lead to fracture with deeply impacted wisdom teeth. [143]
A late mandibular fracture can occur because in very rare cases the removal of a lower wisdom tooth can weaken the jaw bone. Usually this will occur a few weeks after surgery when the patient is feeling better and starts to eat normally as the biting forces can cause a late mandibular fracture. Usually a cracking noise is heard with a mandibular fracture. [33]
Mandible fracture may require stabilization with an intermaxillary fixation or rigid internal fixation of the jaw for 4 to 6 weeks along with antibiotics. [122]
A literature review in 2010 found that at least 128 people have had mandibular fractures occur from removing a wisdom tooth. This is quite small and the reported incidence is 0.0049%. [91, 105]
In one case a woman had 3 impacted wisdom teeth extracted in which she suffered a left mandible fracture. Arch bars and alignment wires were then placed in her mouth. She then had a procedure known as a bilateral ostetomy performed where her jawbone was cut and realigned and then her mouth was again wired shut. [153]
12. Alveolar Process Fracture
It is possible for the lingual plate, alveolar plate, buccal cortical plate, palatal cortical plate, and labial cortical plate(s) to fracture during or after removing a wisdom tooth. The alveolar process contains bone in which the tooth sockets are in. This bone may fracture and this may occur with excessive force and abrupt and awkward extraction movements. [82, 87, 91, 92, 94, 122]
In one case a 25 year old male was having 4 impacted wisdom teeth removed under Lidocaine (local anesthetic). Half-way through the surgery he suddenly jerked his head and this caused the dental drill bur (bit) to perforate the lingual plate (thus causing it's fracture). This severed (damaged) the lingual nerve which resulted in paresthesia (numbness). [114]
In elderly patients, fracture of the alveolar bone may occur more frequently and lead to death. [172]
13. Secondary Infection
Infection following the surgical removal of wisdom teeth happens to about 1 or 2 out of 100 people and is called a secondary infection. Signs of infection include fever above 100 degrees, abnormal swelling, pain or a salty or prolonged bad taste, with or without evidence of discharge from the surgical site.
It is important to practice good dental hygiene and avoid toxic habits such as smoking and drinking alcohol to help prevent infections. [101]
Infection can continue to occur several weeks after wisdom teeth removal if plaque becomes trapped in any extraction site(s). If you have an infection you may need antibiotics and may need drainage performed as well.
14. Periodontal Defects/Damage
It is possible for periodontal pocketing to occur behind an adjacent second molar where a wisdom tooth was extracted. This is possible if the wisdom tooth removed was deeply impacted against the adjacent second molar and there was very little or no bone in between these teeth. This pocket can become a source of inflammation and retention of plaque requiring treatment such as root planing and scaling. A periodontal pocketing forming behind an adjacent second molar where a wisdom tooth was removed could potentially lead to sensitivity in that second molar. [51]
If a person has a healthy wisdom tooth removed they may have a 48% increased risk of developing periodontal pockets. This means gum health can detoriate after wisdom tooth extractions and their is a potential risk of a persistent localized periodontal problem after extraction. [109, 163]
15. Osteomyelitis
Osteomyelitis is an inflammation of bone cortex and marrow that develops in the jaw which can develop as a result of infection of a tooth, periodontal abscess (a collection of pus), by way of transfer from the paranasal sinuses, and trauma. Acute osteomyelitis (occuring less than 1 month) is characterized by a rapid and severe infection with inflammation, intense pain, elevated body temperature, and redness which can be life threatening. The infection can spread and cause extensive throat, and neck swelling which can cause difficulty breathing and may require an emergency tracheotomy to open and preserve the airway to avoid death. The infection can also be deadly if it spreads to the heart and lungs. If the spread of infection is not as severe the symptoms can mimic a prolonged dry socket making it difficult to diagnose and treat. Bone infections can be difficult to cure and typically require long-term intravenous antibiotic therapy, potential hyperbaric oxygen therapy, and sometimes surgery. [17, 36, 48, 130, 140]
A 31 year old man had pain, swelling and difficulty opening his mouth due to a paramandibular abscess. He subsequently receieved intravenous antibiotics and removal of all four wisdom teeth. He developed severe osteomyeltis which required a partial resection (removal) of the mandible and exarticulation (dislocation). [131]
In another case a woman had 1 wisdom tooth removed and returned for the office numerous times complaining of pain and was treated for dry socket. Later she was told that "what has happened is the socket has remained open and infected for so long that [her] jawbone... as a result has died." She had another dentist reopen her gum area and scrape away the dead bone. [154]
16. Osteonecrosis of the Jaw (ONJ) / Medication-related Osteonecrosis of the Jaw (MRONJ)
Osteonecrosis of the jaw can occur after wisdom teeth removal. It is a disease that can cause damage and death to both the maxillary (upper) and mandibular (lower) jaw bone. Bone that is exposed will fail to heal. This necrotic bone can become painful. Osteonecrosis of the jaw is associated with patients taking antiresorptive agents including intravenous (IV) bisphosphonates, oral bisphosphonates, and RANK ligand inhibitor and is also associated with patients taking antiangiogenic agents. One study showed the risk of ONJ occuring in patients exposed to oral bisphosphonates after tooth extraction is 0.5%. [84, 85, 160, 178]
If you are on bisphosphonates such as if you have osteogenesis imperfecta (genetic disorder with very fragile bones), osteoporosis, or some other bone condition, you should notify your dentist and proceed with extreme caution before undergoing any surgery to remove healthy impacted wisdom teeth. [86]
17. Osteoradionecrosis (ORN)
Osteoradionecrosis is a condition that affects bone healing that can lead to death and damage of the jaw bone in someone who has previously received high doses of radiation likely due to head and/or neck cancer treatment or will in the immediate future be receiving radiation in high doses. Hyperbaric oxygen therapy is commonly used prior to any extraction of a patient who has previously had radiation within the last few years. Taking antibiotics before any tooth extraction is also commonly used to help prevent ORN in those patients who have or soon will have radiation of the head and/or neck. [87, 88, 89, 90]
Again, this is a complication that occurs in people who have recieved high doses of radiation or soon will receive high doses of raidation (so it does not affect the average person having a wisdom tooth extracted) and occurs due to the radiation decreasing the bone's blood supply and ability to receive oxygen. The incidence (likelyhood) of ORN after a tooth extraction in patients receiving or soon to receive radiation is estimated to be betweeen 2% and 18%. A literature review in 2010 estimates that 7 in 100 patients who will undergo radiation after a tooth extraction will develop ORN. (Note these statistics are for all tooth extractions and not strictly wisdom tooth extractions). [88, 90]
If you are considering an extraction of a wisdom tooth and have received radiation of the jaw in high doses or plan to be receiving radiation of the jaw in high doses you should notify your dentist. [88]
18. Sequestrum (Small Fragment of Dead Bone) / Bone Spicules
A piece of dead bone known as a sequestrum (squestra is plural form) also known as bony dehiscence can potentially form on the inside of any wisdom tooth extraction site near the tonque. This happens when a small fragment or small fragments of bone break offs from the socket and finds a way to the surface of the gum and protrudes through the gum. Exposed bone that is sharp can lead to the tonque being sore, cause pain, and lead to potential infection. In some cases sequestra can be removed by yourself or left alone if there is minimal irritation as small slivers of bone can work themselves out over time. In other cases an oral surgeon or dentist can remove bone fragments or sharp ridges and smooth out any exposed bone which may require local anesthesia. [51, 52, 82]
19. Herniation of Buccal Fat Pad (Prolapse of Buccal Fat Pad)
The buccal fat pad is found in the cheek between the buccinator muscle and several other superificial muscles such as the masseter muscle. The buccal mucosa and buccinator muscle can tear and cause the buccal fat pad to protrude into the oral cavity which is known as herniation of the buccal fat pad and prolapse of the buccal fat pad. A lipoma can result which is a benign fatty tumor. [17, 27, 38]
20. Tooth Root Fracture
A root can sometimes fracture during the extraction of a wisdom tooth. If this does happen the surgeon will usually see it and remove it. In other cases it can become displaced.
21. Injury to Adjacent Teeth
Teeth and tissue next to (adjacent) the wisdom tooth extracted can be damaged during surgery and so can any fillings, crowns, and/or bridges (known as restorations) that were previously done. Hence a previous dental carie (cavity) that may have been restored through the use of porcelain, dental amalgam, gold, or composite resin in a second molar next to the third molar that is being removed could be damaged. This could require additional treatment and a new restoration to be placed.
It is also possible that teeth on the opposite side of the arch (as in if the tooth being extracted on the bottom, the tooth directly above it on the top) could be injured. This can occur with excessive tractional forces by forceps. [82]
It is also possible for luxation of an adjacent tooth to occur which means it becomes dislocated within the socket but continues to have some attachment. Sometimes all that is needed is to simply push the tooth back into the socket and allow for healing to occur. However, in some cases stabilizing the tooth with rigid fixation (such as sutures, arch bars, dental wires, and composite splints) may be necessary to keep it in place. [82, 143] The luxation of an adjacent tooth may need to be stabilized for around 40 to 60 days. [122]
22. Displacement of Root Fragments
It is possible for a root fragment to be displaced which means removed from where it should be but still inside the person's body. You might need to have the fragment removed if it causes problems. Usually the fragment is close to a nerve or adjacent sinus such as the maxillary sinus. Removal of the root tip could jeopardize adjacent structures. The oral surgeon uses his clinical expertise to determine the benefit to risk ratio of removing a root tip. The fragments can be monitored using x-rays.
If a root fragment ends up in the sinus, irrigation with saline may allow the tooth fragment to be brought back to the site of the opening and hence may be retrievable. At other times a procedure called a caldwell luc must be performed. In some cases small root and tooth fragments can emerge on their own after several weeks and may be retrievable by yourself or with assistance from your dentist or oral surgeon. [127, 128]
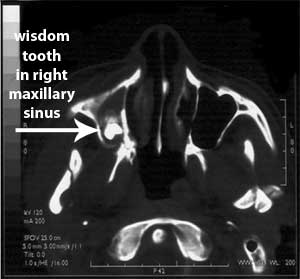
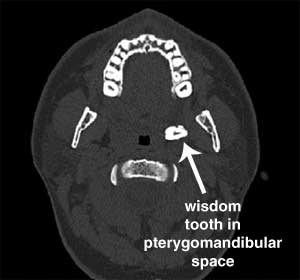
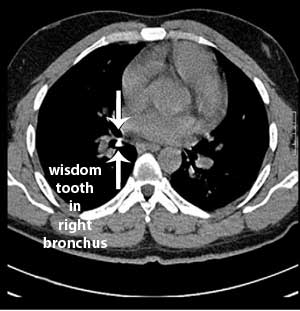
23. Displacement of a Tooth
It is also possible for a tooth to be displaced with means removed from where it should be but still inside the person's body. The tooth could go into the numerous locations including the maxillary sinus, infratemporal fossa, submandibular space, pterygomandibular space, lateral pharyngeal space, lateral cervical region, and buccal space. It is even possible for a tooth to be aspirated and end up in the respiratory tract. A tooth in the airway can cause aspiration pneuomonitis, leukopenia, pneuomonia, and could lead to death. A tooth can also be swallowed and pass through the gastrointestinal (GI) tract. A tooth in the GI tract will likely pass several days after being swallowed and thus end up in the toilet when going to the bathroom. [44, 59, 64, 82, 159, 174]
For a patient with displacement of a root fragment or tooth into the maxillary sinus, irrigation with saline may allow the root fragment or tooth to be brought back to the site of the opening through which it entered the sinus, and may be retrievable. At other times a procedure called a caldwell luc must be performed. [34]
A patient with a displaced maxillary wisdom tooth into the infratemporal fossa either has no symptoms or has symptoms of a chronic infection. A wisdom tooth displaced into the infratemporal fossa can be very difficult to remove and could cause hemorrhage or neurological injury without actually getting the tooth out. Antibiotics, radiological imaging, and surgery may be needed however there is no universal treatment. [27, 37]

A 27 year old man underwent a lower left wisdom tooth extraction in the U.S. that was not properly extracted. A few months later he visited an oral and maxillofacial surgeon in the U.K. He complained of pain and reduced ability to open his mouth. A CT scan that was performed showed a tooth and tooth fragment present between his tonsillar soft tissue and medial pterygoid space. The wisdom tooth and tooth fragment were sucessfully retrieved under general anesthesia. [126]
A 23 year old man had a symptomatic partially impacted lower left wisdom tooth removed under local anesthesia. Surgery caused the man to have a gag reflex in which the tooth disappeared. He had a chest x-ray and CT scan performed which showed his wisdom tooth ended up in the right bronchus which is the airway leading into the lungs. Bronchoscopy was performed under general anaesthesia in order to remove the wisdom tooth. [59]
In another case, a 20 year old woman had all four impacted wisdom teeth removed while receiving nitrous oxide, diazepam, and meperidine. While one of the wisdom teeth was being removed she jerked and the wisdom tooth went down her pharynx. A chest x-ray showed the wisdom tooth in her right bronchus. Bronchoscopy removed the wisdom tooth. [97]
24. Displacement of a Foreign Body (Dental Instrument)
It is possible for a dental instrument such as a the blade of an elevator, drill burr, or anesthesia needle to break during surgery. A piece of gauze could also become lodged in the airway and potentially lead to death or be left in and lead to infection. [98, 104, 122, 144]
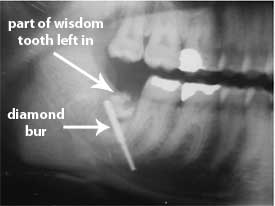
A 35 year old woman had her right mandibular wisdom tooth removed and 3 weeks later complained of difficulty opening her mouth, swelling, and pain. A panoramic radiograph showed that part of the wisdom tooth and a foreign body were left in the socket. A CT showed the foreign body in the submandibular space. She underwent surgery to have the rest of the wisdom tooth extracted and the foreign body. The foreign body was a 20-mm long diamond bur which is a dental drill bit. [28]
In a case in Texas a woman had her third molars removed and had her lingual nerve bilateraly severed and the drill burr broke in her mouth. The dentist was unable to find the broken piece and did not bother to inform her of this. Years later the broken piece of the dental drill bit continues to remain in her mouth. [156]
A dentist bent a 27-gauge needle before insertion to adminsiter a local anesthetic to the right inferior alveolar nerve in a 21 year old male having his wisdom teeth removed. A three-dimensional (3D) image of the needle portion that had broken off into the man's mouth (oral cavity) was obtained by using both a panoramic radiograph and a computed tomography (CT) scan. He was hospitalized and a surgeon removed the needle while he was under general anesthesia. [69]
In another case a dentist was injecting a local anesthetic in a 20 year old female who was having her lower wisdom teeth removed when the 30-gauge short broke at the hub which is the section where the metal needle meets the body of the syringe. The dentist attempted to retrieve the approximately one inch fragment of the metal needle but was unable to. He then put her in a car and drove her to an oral surgeon who was also unable to remove the fragment. A surgical attempt to remove the fragment at a hospital also failed. The patient sued the dentist but a jury found the dentist not negligent. [70]
Surgery to retrieve a fragment of a needle that has fractured can be lengthy. In one case the operation time was 2 and a half hours. [123]
In another case in Italy, a 24 year old man had a 25-mm 30-gauge dental needle break off during an inferior alveolar nerve block while having a lower left wisdom tooth extracted. The man had the needle successfully retrieved under general anesthesia through the use of a computer-based image-guided system. [173]
There are certain steps that dentists can take to help avoid needle fractures. These include avoiding the use of 30-gauge needles to administer inferior alveolar nerve blocks, avoiding the use of a short needle to administer inferior alveolar nerve blocks as it likely will be inserted up to the hub, avoiding bending the needle prior to insertion, and avoiding burying the needle in the tissue to the extent that the hub indents the mucosa. If a needle does break antibiotics should be prescribed, a panoramic radiograph should be obtained, and the patient should avoid opening his or her mouth widely, such as with chewing and swallowing, so as to limit the needle fragment's potential movement. Oral and maxillofacial surgeons generally recommend removing the broken needle as soon as possible. A 3D CT scan is recommended to accurately determine the needle's position and the operation to remove a needle fragment should be performed under general anesthesia. [69, 71]
Anyone who is having a local anesthetic injection should understand that if they suddenly move when the injection is being administered this can contribute to a needle breaking and thus a fragment being left in the mouth. Also of note is the majority of needle fractures occur during inferior alveolar nerve block. [69, 71]
A literature review in 2010 from 1965 until when the study was published found that at least 64 needles have been broken in the mouth after local anesthesia. Needle fractures can be occasionally due to faulty manufacture and thus the fault lies with the needle manufacturer, but usually is due to inadequate technique or using too thin of needles. [69, 70, 71]
A man had two wisdom teeth extracted in 1978, in Mississippi, in which the dentist packed the cavity with gauze. He later returned over a month a later complaining of numbness and feeling a material still in the socket. The dentist removed a piece of gauze from a hole in the man's jaw which he had overlooked at an earlier follow up visit. [149]
A woman had two wisdom teeth extracted in 2004, in New York, by an oral surgeon. Three days later she returned to the office complaining of severe pain. Four days after that she went to a different dental clinic complaining of pain around the lower extraction socket and the doctor removed the packing. The woman and her mother insisted that there was also packing in the upper socket but the doctor could not find any. The woman continued to have right maxillary sinus pain and earache for over a month and hence a panoramic radiograph and exploratory surgery were performed. Roughly 2 months after the extractions the woman had a small piece of gauze come out of her right nostril. Two days after this more gauze came out of her nose. She then had a CT scan of her sinus with showed an area of density in the right maxillary sinus. The woman went to an ear, nose, and throat specialist who performed sinus surgery and allegedly removed gauze from her right maxillary sinus. She had two subsequent sinus surgeries and suffers from chronic sinus infections and loss of vision in her right eye. [151]
25. Foreign Body Granulomatous Reaction
It is possible to develop a granulomatous reaction following wisdom teeth removal which is when the immune system attempts to fight a foreign body that is present. The granuloma can occur in the tooth extraction socket and could be caused by bone wax. Reactions to bone wax can cause persistent giant cell inflammation, delayed bone healing, and potential infection. Bone wax is used to stop bleeding and alternatives such as Surgicel are available. Hence non-resorbing materials should be used in close proximity to nerve areas such as in the extraction socket. [83, 161]
In one case a 29 year old woman complained of numbness in her right mental nerve that was worsening. Eleven (11) years prior she had had her lower wisdom teeth extracted and had had numbness for a month afterwards which spontaneously resolved. She had a CT scan of her mandible which showed a rounded expansion suggesting a neuroma in the right inferior alveolar canal. Several months later when she began to also experience pain, surgical exploration occured which revealed and allowed for the removal of a large piece of bone wax. A year after surgery she no longer had pain and began to regain some sensation in the right mental nerve. [83]
26. Wrong Tooth and/or Wrong Teeth Extracted
It is possible to have the wrong tooth and/or even the wrong teeth extracted when undergoing surgery to remove a wisdom tooth. [61, 62] It is even possible for a surgeon to deliberately pull more teeth than what you consented to, so they can make more money, although certainly negligent. [103]
In one case a 20 year old female was referred from her orthodontist to a surgeon to have her lower wisdom teeth removed. The orthodontist wanted to have the upper wisdom teeth kept to help provide anchorage and have them extracted later. The surgeon removed both the upper and lower wisdom teeth on the left side. It is noted that due to such the common practice of removing all four wisdom teeth at once the surgeon was confused! [61]
In another case a 13 year old boy was supposed to have two wisdom teeth removed but instead the oral surgeon mistakenly removed two healthy permanent teeth. [112]
27. Negative Exploration - Drilling in the Area where a Wisdom Tooth is not Present
It is possible for the panoramic x-ray left and right to be mislabeled and/or for the surgeon to mistakenly attempt to drill and remove a wisdom tooth that is not present on the left side of the mouth but actually is present on the right side of the mouth or vice versa. This could happen in cases where a patient has 3 impacted wisdom teeth instead of 4 impacted wisdom teeth. Thus the surgeon may start to drill for a wisdom tooth that is typically present with 4 wisdom teeth present but is not present with only 3 wisdom teeth. Other potential possibilities are of course possible. [138]
In one case a man had 3 impacted wisdom teeth present and underwent surgery to have them extracted. The surgeon removed the two upper wisdom teeth and then proceeded to remove the third wisdom tooth. The surgeon drilled by mistake on the lower left side when the wisdom tooth was actually on the lower right side. In the process this lead to the man to suffer from continued numbness in the area of the jaw, chin, and lip on the lower left side where there was never any wisdom tooth present. The court documents from this case say "it is at least arguable that an oral surgeon's act of drilling on the wrong side of a patient's mouth is akin to a surgeon's amputation of the wrong limb." [138]
28. Inadvertent Removal of Tooth Next to Wisdom Tooth
It is possible that while undergoing surgery to remove a wisdom tooth, a tooth adjacent to a wisdom tooth also becomes extracted. This could be the result of concrescence which is an uncommon anomaly that can be described as the union of adjacent teeth involving only the cementum which is a substance which covers the root of a tooth. Concrescence most often affects maxillary (upper) third molars (wisdom teeth) and second molars. [93, 94]
Concrescence can be very difficult to identify on a radiograph. Having numerous radiographs taken from different angles and with different exposure parameters may help detect concrescence but even then it can still be difficult to determine. Hence since concrescence is so rare and very difficult to diagnose before surgery, an oral surgeon may make the diagnosis halfway through extracting a tooth and then find it necessary to also have to extract the second molar next to the wisdom tooth due to the solid cemental attachment between the two teeth. Hence if multiple radiographs do not produce clear images for detection of concrescence, cone-beam computed tomography should be used to aid in diagnosis. [93, 94, 95]
It is important to know that if an extraction is performed on a wisdom tooth that is concrescent, certain complications such as maxillary sinus exposure and fractures are more likely to occur. [93, 94]
29. Myositis Ossificans
It is possible to develop myositis ossificans where bone forms within skeletal muscle or soft tissue. This can occur if a root or tooth fragment is displaced and subsequent surgery to remove the displaced root or tooth fragment leads to muscle trauma. [55, 60]
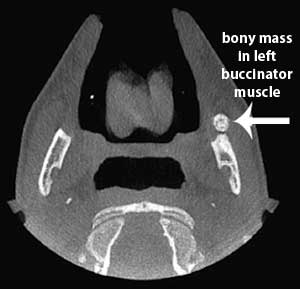
A 17 year old male complained of a constant dull aching near the anterior border of his left mandible ramus which started after he had his wisdom teeth removed and progressively worsened over 18 months. He had a decreased range of jaw movement. A cone-bean CT showed a bony mass in his left buccinator muscle. Surgery removed the mass. He recovered and regained full range of jaw movement. [55]
In another case an 18 year old female had 4 wisdom teeth removed under general anaesthesia. One week later she returned to the surgeon complaining of muscle soreness when opening her mouth. For several months it was not known what was going on until a CT scan showed calcification of the right medial pterygoid and temporalis muscles which indicated she had myositis ossificans. She had three subsequent surgeries performed and continuous follow-up for over 5 years after the original extractions. The plan is to give her a prosthetic joint once her myositis ossificans is in remission for a long period of time. [60]
30. Temporomandibular Joint Syndrome (TMJ) dysfunction
TMJ (jaw joint) dysfunction following the removal of wisdom teeth is unusual and usually temporary. If treatment is required, it is usually conservative in nature and includes anti-inflammatory medicines, physical therapy, rest, heat, and in some cases short term bite splint therapy. It is possible for the their to be pain, locking, soreness, and/or tenderness in the jaw joint which could potentially be permanent. The Temporomandibular Joint can dislocate which can be caused by the surgeon opening the mouth excessively during extraction. [122]
Learn more about TMJ dysfunction after wisdom teeth removal.
31. Life-Threatening Hemorrhage (Excessive Bleeding)
It is possible to literally bleed to death after wisdom teeth removal. The most common reasons to experience hemorrhage after wisdom teeth removal is due to soft-tissue and vessel injury. The hemorrhage could occur due to injury to the lingual artery or one of its branches. Hemmorhage may occur more often with mandibular wisdom teeth. [143]
Hemorrhage could also occur in someone who has not had surgery before and does not know they have a systemic cause that could lead to hemorrhage. Hence, any family history of bleeding abnormalities should be told to the surgeon. In these cases hemorrhage could be due to medication that affects coagulation, coagulation disorders, liver disease, and hypertension. [8, 143]
The main methods of stopping bleeding include compression, suturing, electrocoagulation, ligation, and using hemostatic materials. [122]
A 14 year old girl had 4 wisdom teeth extracted. She had on and off bleeding for 10 days after and was brought to an emergency room. She suffered cardiac arrest in the hospital waiting room due to the large amount of blood she had lost. She was successfully resuscitated and recovered. [140]
A 61 year old male had an impacted mandibular third molar removed. He lost around 2 L of blood and had to be transported to a medical center before it could be controlled with embolization. [176]
See the Death section below for a description of a case of a man who bled to death after oral surgery.
32. Headache
You could develop a headache. This headache could be temporary or could be chronic and permanent. As stated above under the mouth-sinus hole complication (#5 above), a sinus infection due to penetration of the maxillary sinus cavity during widom teeth removal can potentially cause a long lasting headache.
It is possible that this headache is a rare entity known as new daily persistent headache (NDPH). NDPH is a daily, unremitting headache which occurs from the onset. The pain is usually bilateral, pressing or tightening, and of mild to moderate intensity. It occurs in patients who have no significant headache problems in their past. It is known that surgery, viral infections, and stressful life events are triggers for the onsent of NDPH. [5, 66, 67, 68]
An extremely interesting observation is that in rare cases patients will wake up after extracranial surgery such as having their appendix removed (appendectomy) with new daily persistent headache. The appendix is considered to be a vestigial structure just like wisdom teeth meaning that they are believed to have had use for our ancestors but have lost their orginal function for us today through evolution. It used to be that almost everyone would have their appendix removed when they were still young. Nowadays a healthy appendix is not removed due to the risks of surgery. [66, 67, 68]
The website's owner developed a 24/7 headache which causes him severe pain every day. See the about me page if you haven't yet seen it.
In the scientific literature there is a case report of a 48 year old man who had an upper left wisdom tooth extracted and two weeks after began to experience left side severe headache attacks. He had absolutely no history of headache and no dental pain prior to the extraction. He experienced cluster headaches after the wisdom tooth was extracted. He was given oxygen and prednisolone intially. Then he was given verapamile and litium carbonate as a preventative which helped to reduce the frequency of the cluster headache attacks. [111]
A possible reason given for the 48 year old man who developed cluster headache after having a wisdom tooth extracted is described in Soros 2001. Teeth are innervated by unmyelinated C fibres which project to the trigeminal subnucelus caudalis of the brainstem. "Experimental tooth pulp denervation is known to result in a hyperactivity and in expanded receptive fields of neurones in the trigeminal nuclei. Reorganizational changes start within minutes or days after deafferentation of teeth...phantom tooth pain does not necessary begin immediately after...tooth extraction. The delayed onset of phantom pain suggests that, in many patients, reorganizational changes need to evolve until they have perceptual consequences...It might be possible that the ongoing reorganization of spinal and brain stem networks induced by the irritation or deafferentation of C fibres contributed to hypothalamic reorganization." [111]
Make sure you also see wisdom teeth removal stories shared by others for additional case reports on headaches occuring after wisdom teeth extractions.
33. Hematoma
A hematoma is a localized collection of blood outside the blood vessels (vascular system) and within tissues that is caused by prolonged capillary hemorrhage (bleeding). [122] A hematoma could be due to the dentist or surgeon improperly injecting local anesthestic. [140]
It is possible that if a hematoma forms around the airway than it can lead to respiratory problems. If a hematoma forms around the eye, as in intraorbital hematoma, it does carry a significant risk of blindness. [45]
A 21 year old man developed an intraorbital hematoma after having both of his upper wisdom teeth removed under intravenous sedation with midazolam. He developed swelling around his left eye. He was given intravenous antibiotics, Bacitracin ophthalmic ointment, Lacrilube, an eye shield, and Timoptic drops. On a one month follow up he had no functional problems. [45]
A 19 year old man had four impacted wisdom teeth removed under anesthesia. He then developed a retrobulbar hematoma confined to the extraconal space. The hematoma caused periorbital swelling and ecchymosis with evidence of proptosis and swelling of the right check. The hematoma was drained and he gradually recovered. It was hypothezied that a branch of the posterior superior alveolar artery was damaged and bleeding tracked through the pterygomaxillary fissure into the pterygopalatine fossa and eventually drained into the retro-orbital space via the inferior orbital fissure. [177]
See the Death section for a description of a person who died from airway obstruction from a postextraction hematoma. [20]
34. Facial Artery Pseudoaneurysm
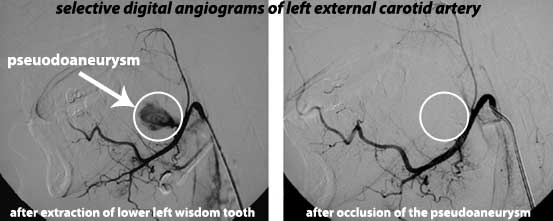
It is possible for a pseudoaneurysm which is a false aneurysm to develop. A pseuodaneurysm is a pulsating hematoma that forms due to a rupture in an artery. Removing wisdom teeth can damage the facial artery wall which can cause a psuedoaneurysm due to blood flowing and staying in surrounding tissues. This can lead to life-threatening hemorrhage. Computed tomographic angiography aids in detection and treatment includes controlling hemorrhage and removing the lesion. [41]
A 25 year old man developed a psuedoaneurysm in a proximal branch of the left proximal facial artery with surrounding hematoma after extraction of his lower left wisdom tooth. Cannulization of the left facial artery was performed and iodized oil and n-Butyl-2-Cyanoacrylate_histoacryl was injected into the left facial artery with a microcatheter. This allowed for the pseuodoaneurysm and adjacent parent artery to be occluded. Twelve months later the patient's only complaint was mild left lingual paresthesia. [39]
35. Myoclonus
There is some literature suggesting peripheral nerve damage causes myoclonus and body pounding symptoms/ palpitations.
36. Brain Damage
Anesthetics have been linked both mechanistically and phenomenologically to brain damage in non humans. A few people have noticed cognitive impairment after recieving anesthesia. Lack of oxygen to the brain during surgery can lead to brain damage. Being given an overdose of anesthesia has caused brain damage in many cases. [141]
A 17 year old high school boy in Kansas suffered brain injuries (partial blindness and neurological problems) as a result of a faulty medical gas system that had the nitrous oxide and oxygen lines switched while having his wisdom teeth removed. See https://blog.teethremoval.com/family-reaches-3-million-settlement-from-faulty-medical-gas-during-wisdom-teeth-surgery/ for more information.
In another case a woman in Texas was given an overdose of sedation and suffered permanent brain damage. The court documents say she "went from being an accomplished pianist and equestrienne to one who is now challenged in these and in many other areas." [155] See also https://blog.teethremoval.com/wisdom-teeth-removal-can-lead-to-brain-damage/
In another case a 36 year old woman in Indiana went into a coma for 10 days as a result of an overdose of anesthesia after having her wisdom teeth removed that left her brain damaged. This resulted in her needing a live in sitter, being virtually unresponsive, and not even aware of how old her daughter is. [117]
In another case a man in 1984, in Wyoming, was given four drugs to take prior to surgery of his wisdom teeth. One of these drugs included taking "atropine 1/4 grain take 1/2 hour before dental appt." The man took the prescriptions to the pharmacist to have them filled. The pharmacist observed the excessive dosage in the atropine prescription and called the dentist to discuss. The dentist refused to discuss the prescription with the pharmacist and requested the pharmacist fill the prescription as written. The pharmacist did and gave the prescription to the man who took all 25 atropine capsules. Prior to surgery the dentist realized that the man had taken a toxic dosage of atropine. Instead of calling Poison Control as was advised after discussing with a medical doctor the dentist proceded with the surgery to remove the wisdom teeth and did not call Poision Control until more than 24 hours later. The dentist also did not tell the man or his mother about the overdose. On his way home from the extractions the man began to hallucinate and manifest unusual behavior. Eventually the man ran away from his family ranch house and thought he saw men chasing him with guns and shining lights on him. During his hallucinations, he broke his glasses, ran into a barbed wire fence and got wet running through a creek. He also suffered a serious knee injury when he stepped off the top of a hill and fell forward through the snow. He eventually made it to his neighbor's ranch house roughly two and one-half miles from his house and slept the night in a haystack. The next morning the man was still hallucinating and thought he saw men who were after him blow up the haystack next to the one he was in. He had to later have arthroscopic surgery and years later continues to have trouble remembering things and a volatile temper. [157]
See the Death section below for a description of some individuals who were left brain dead after having their wisdom teeth removed.
37. Necrotizing Fasciitis
It is possible to suffer a potentially deadly aggressive bacterial infection called necrotizing fasciitis which is commonly known as flesh-eating disease. This can appear as a red, hot, painful, and swollen wound with an ill-defined border of ecchymosis. If this complication occurs it usually appears 2 to 4 days after surgery. This can occur in combintation with sepsis which is where the whole body is in an inflammatory state due to being overwhelmed with bacteria. Immediate treatment with surgery and antibiotics is needed. The mortality rate is reported in several studies as quite high with several studies having reported rates in the mid thirty percents. [164]
A healthy 14 year old man elected to have his wisdom teeth removed under conscious sedation. Two days after he had a temperature of 100 degrees Fahrenheit or 37.9 degrees Celcius and redness around the eye (periorbital erythema). Over the next 24 hours this erythema extended to his right neck and anterior chest wall and he went to the emergency room. He was diagnosed with multiple fascial space infections and given intravenous antibiotics and underwent surgical drainage. He had to be airlifted to another hospital and arrived in septic shock. He was given hyperbaric oxygen treatment, an antibiotic treatment, and skin grafting done on his neck and chest. The images from this occuring are extremely graphic. [40]
See the Death section below for a man who died from necrotizing fasciitis after wisdom teeth removal.
38. Air Embolism
A gas related embolus can be caused by inadvertent injection of a mixture of air and water under pressure which then passes into the mandible (jaw) to the veins and then to the large vessels leading to the heart. Large amounts of air can cause serious problems including cardiac arrest and death, by traveling to the large veins leading to the heart, and mechanically blocking the flow of blood through the heart. Microbubbles, not detectable by conventional imaging techniques may provoke an inflammatory response and cause tissue damage. Doppler ultrasound may aid in detection and hyperbaric oxygen therapy for treatment. [3, 7]

39. Subcutaneous or Submucosal Emphysema
Subcutaneous emphysema results when air is forced beneath the dermis which is a layer of skin between the epidermis and subcutaneous tissues. [19] It stems from an injection of air and/or water can which result from the use of an air-water-cooled high-speed dental handpiece to extract a wisdom tooth. Although not confined just to wisdom tooth extractions, over 75 cases of subcutaneous emphysema have been reported in the literature from dental extractions. [21, 122]
A 32 year old woman developed subcutaneous emphysema after wisdom tooth extraction and began complaining of swelling and pain over her left face and neck and difficulty swallowing. A CT scan showed air accumulation in the left infratemporal space, pterygomandibular space, buccal space, masseteric space, upper part of the parapharyngeal and retropharyngeal space, along the deep cervica fascia, and extending to the anterior wall of the chest. She was given several antibiotics and an incision and drainage at the left submandibular area was peformed to prevent the extension of air into the mediastinum. After a 2 week follow up she had no complaints. [21]
40. Pneumomediastinum
Pneumomediastinum is when there is air in the space between the lungs known as the mediastinum. It is caused by air driven drills just like subcutaneous emphysema but usually when more air is present. [19]
A 32 year old woman developed subcutaneous emphysema and pneuomediastinum after extraction of an impacted third molar of which an air driven drill was used to section the tooth for removal. Six hours after the surgery she had neck and facial swelling and the following morning had more chest, neck, and facial swelling. X-rays and a CT scan were performed and she was given cephalexin monohydrate (an antibiotic) and acetaminophen (pain reliever). Thus conservative treatment was followed and after 2 weeks the subcutaneous emphysema and pneumomediastinum had cleared up. [19]
A literature review in 1993, found that there were thus far at least 13 cases of pneumomediastinum associated with wisdom teeth removal. Numerous cases have since been known since then like the case described above and below. [47, 121]
41. Pneumothorax
If a really large amount of air is injected from an air driven drill, even more than in pneumomediastinum and subcutaneous emphysema, then a pneumothorax which is a collection of air in the space around the lungs, also known as a collapsed lung, can result. [19, 29]
A 45 year old man had his right lower second molar and left lower third molar extracted under intravenous sedation. An air turbine dental handpiece was used to remove bone and to section the tooth during which the patient complained of chest pressure. Surgery was stopped as severe subcutaneous emphyesema was seen. A CT scan showed that bilateral pneumothorax and pneumomediastinum was present. Surgical drainage was performed and the man was given antibiotics. After 4 days his symptoms went away. [29]
42. Descending Necrotizing Mediastinitis
Mediastinitis is the inflammation due to infection of the tissues in the space between the lungs known as the mediastinum. Descending necrotizing mediastinitis can occur due to an infection in the oral airway. The oral airway infection (oropharyngeal infection) spreads to the fascial spaces of the head and neck and then extends down into the mediastinum. Surgery may need to be performed to drain fluid collections such as abscesses that have formed and antibiotics are needed for treatment. [43, 133]
A 23 year old woman developed mediastinitis with a fistula to the left main bronchus after having her wisdom teeth removed. [11]
In another case a 23 year old man had four wisdom teeth extracted under conscious sedation. Five days after the extractions, he had swelling, difficulty opening his mouth, and a fever of 103.5 Fahrenheit or 39.7 degress Celcius. A CT scan showed edema of the left submandibular and parapharyngeal spaces. He was given intravenous antibiotics and fluid from these spaces were drained. He had underwent thoracotomy and mediastinal exploration 3 different times and required hospitalization for 26 days. He had developed descending necrotizing mediastinitis and Lemierre syndrome from getting his wisdom teeth out; however, he eventually made a full recovery. [43]
43. Lemierre's Syndrome
Lemierre's Syndrome starts with an infection in the head and neck region. The infection then spreads to a space in the neck known as the parapharyngeal space. Here blood vessels become infected and then the infection moves to the internal jugular vein. The formation of a blood clot (thrombus) occurs. The inflammation of vein (thrombophlebitis) related to the blood clot (thrombus) can cause septic emboli which are emboli infected with bacteria. These septic emboli can then spread to other organs and parts of the body causing complications of the central nervous system and pulmonary or other manifestations including septic shock. This very rare disease is known to affect young and healthy adults who are most likely the ones having their wisdom teeth taken out. Surgical drainage and intravenous antibiotics are usually needed for treatment. [9, 10]
Symptoms of Lemierre's Syndrome vary from person to person but typically consist of a high fever, neck pain, swelling, and a sore throat. The mortality rate of Lemierre's Syndrome is in the range from 0% to 18% even if the condition is quickly treated. [10] Read https://blog.teethremoval.com/near-death-wisdom-teeth-removalexperience/ for a description of a 17 year old girl who was left paralyzed, suffered several strokes, and nearly died as a result of Lemierre's Syndrome while having her wisdom teeth removed.
44. Ludwig's Angina
Ludwig's angina is a rapidly spreading infection in the floor of the mouth. It is typically seen in infected wisdom teeth that have not been extracted that affects the submandibular space by spreading directly through the fascial planes causing the surrounding gums to become infected. However, Ludwig's angina can occur following a tooth extraction when bacteria from the mouth get in to tissues under the mandible (jaw). The infection spreads and causes difficulty swallowing, trouble breathing, swelling, severe pain, drooling, and elevated temperature. Ludwig's angina can lead to asphyxiation and death. Treatment includes intravenous antibiotics and surgical decompression (drainage) of the spaces of infection (submandibular, sublingual, and submental) may be needed as well. [9, 42, 102, 119, 122]
A 29 year old woman arrived at the emergency room complaining of severe pain and swelling in her lower jaw which was four days after the extraction of 3 wisdom teeth. She had a temperature of 103.6 degrees Fahrenheit or 39.8 degrees Celcius. She was given intravenous antibiotics and had a procedure known as a tracheotomy to allow air through her neck. Later the soft tissues in her neck were decompressed. She stayed in a hospital for 8 days while continuing intravenous antibiotics before being discharged and sent home. [65]
A 21 year old man developed Ludwig's angina following a wisdom tooth extraction in the early 2000's. He had head, neck, and chest swelling and was treated in a hospital. [102]
A woman had her left wisdom teeth extracted in 1993. Four days later she developed severe pain. Roughly one week later she went to the emergency room for treatment and was diagnosed with a severe infection in her jaw and throat. She was hospitalized for 6 days and had surgical drainage performed. Several years later it was reported that "she continues to suffer from headaches, numbness in her jaw, and a mild speech impediment as a result of the infection." [142]
See the Death section below for a man who died after developing Ludwig's angina following having his four wisdom teeth extracted.
45. Orbital Cellulitis/ Orbital Abscess
Orbital cellulitis or orbital abscess is an infection of the tissues surrounding the eye which could potentially be caused by sinusitus. In some cases a wisdom tooth extraction can lead to an infection which can extend into the orbital and periorbital spaces causing an orbital abscess. [58]
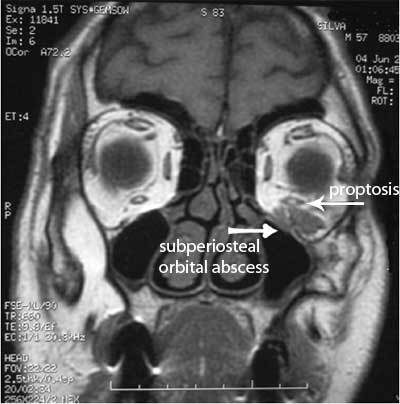
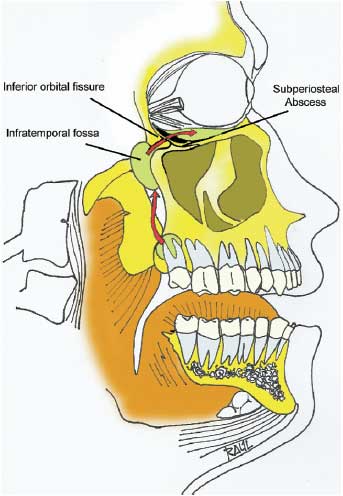
A 57 year old man had an upper left wisdom tooth removed and 5 days later was in the emergency room due to fever, discomfort, redness (erythema) and an abnormal accumulation of fluid beneath the skin beneath the left eye (edema), and eye dislocation (proptosis). He was given intravenous antibiotics. An echogram, CT, and MRI were taken and the MRI confirmed a subperiosteal orbital abscess which is a specific condition of orbital cellulitis. Surgical drainage was performed and the antibiotic treatment was altered based on microbiology culture. One month later the patient no longer had a subperiosteal orbital abscess. [22]
The cause of the subperiosteal orbital abscess likely resulted from an infection which traveled from the extracted wisdom tooth toward the posterior region of the maxilla to the infratemporal fossa and through the inferior orbital fissure to the subperiosteal region of the orbit. [22]
In another case, a 21 year old man had swelling in his left check and periorbital region when he arrived at a clinic 5 days after having his four wisdom teeth removed. He was given intravenous antibiotics and found to have an orbital abscess via a CT. Surgical drainage was performed under general anaesthesia, a microbiology culture was taken, and intravenous antibiotics were continued. After 3 weeks swelling and eye dislocation had resolved. [58]
46. Subdural Empyema
Subdural empyema is a infection that has spread to the subdural space which is one of the layers of tissue between the dura mater and arachnoid matter that covers the brain. The infection causes a fluid-filled mass to form which is filled with puss which is also known as an abscess. Fever, headache, and neck stiffness typically present and if left untreated can progress to lethargy and coma and potentially lead to death.
A healthy 21 year old man developed right-sided Bell's palsy, which is the dysfunction of the cranial nerve and inability to control facial muscles, 4 days after having his wisdom teeth removed. Two days later he was admitted to the hospital with vomiting, facial swelling, inability to normally open the mouth (trismus), elevated white blood cell count, and a temperature of 102 degrees Fahrenheit or 38.9 degrees Celcius. A CT scan was performed and showed an abscess of which was surgically drained. He also was given several different antibiotics intravenously. 24 hours later he developed a severe frontal headache, vomiting, and became drowsy. An MRI was performed (see image below) which showed fluid in the right subdural space. He then developed facial weakness and seizures on the left side of his face. He had an emergency procedure known as a burr hole craniotomy and subdural drainage performed. [12]

47. Epidural Abscess
It is possible to have an epidural abscess which is caused by an infection in the area between the bones of the skull or spine and the membranes covering the brain and spinal cord.
A 20 year old woman complained of neck pain 3 days after extraction of a wisdom tooth under general anesthesia. The epidural abscess went unoticed until 9 days after the extraction when she began to develop partial paralysis in her right arm and right leg and later in the day partial paralysis in her left arm and left leg. She had an MRI done which revealed the epidural abscess to the right side of the C4/C5 vertebrae. She was given intravenous antibiotics and a neurosurgical team performed drainage of the abscess and spinal cord decompression. She regained recovery in her left arm and left leg but continued to have paralysis in her right arm and right leg. [18]
48. Submasseteric Abscess
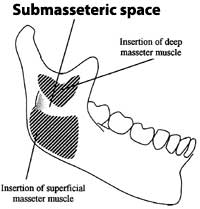
It is possible to have a submasseteric abscess which is an infection in the submasseteric space. The submassetric space is cleft-shaped and is located between the masseter muscle and the lateral surface of the ramus of the mandible. [122]
A 24 year old man had a wisdom tooth removed and had facial swelling occur several weeks later. A CT scan revealed a small abscess beneath the right masseter muscle. He had a fever and a high white blood cell count. Surgical drainage was performed and he was treated with intravenous antibiotics after bacterial culturals were obtained during drainage. He recovered successfully. [23]
In another case, a 22 year old woman complained of tenderness 2 weeks after having her left maxillary third molar extracted. After 3 weeks her condition worsened and she was unable to eat or sleep due to pain and being unable to open her mouth. Blood tests revealed an infection and she had an MRI performed. However awaiting the results of the MRI scan, she developed paraesthesia of the maxillary and mandibular divisions of the left trigeminal nerve and an ultrasound scan of the left cheek was taken which showed a large submasseteric collection. Drainage of the left submasseteric space was performed and she was treated with antibiotics. She likely developed a hematoma in the infratemporal fossa which became infected which spread to the submasseteric space. [24]
49. Brain Abscess
It is possible to have a brain abscess which is a collection of infected material within the brain tissue.
A 26 year old man developed cervico-facial cellulitis with brain abscess after having his mandibular right wisdom tooth extracted. He had emergency neurosurgery and was given antibiotics for 8 weeks. He was left with aftereffects which consisted of jaw constriction and sensory disorders of the right thigh. [26]
50. Cavernous Sinus Thrombosis
Cavernous sinus thrombosis is when a blood clot forms in the cavity located at the base of the brain called the cavernous sinus. Cavernous sinus thrombosis can spread to other venous sinuses, cerebral veins, and meninges. [46]
A 60 year old man with an infected upper wisdom tooth developed cavernous sinus thrombosis 38 days after extraction. [30]
See the Death section for cases where a person died after getting cavernous sinus thrombosis from wisdom teeth removal.
51. Other Fascial Space Infections / Abscess Formation
Wisdom teeth are located near many different fascial spaces in the head and neck where infections can result and bacteria (mostly anaerobic) can spread. An infection can result in an abscess (a collection of pus) formation. Infection can rapidly spread between fascial spaces. The infection could potentially compromise the airway and antibiotic therapy, taking a sample for culture to identify the bacteria, surgical drainage, and securing the airway will be needed. Potential spaces of involvement can potentially include the primary mandibular spaces (consisting of the sublingual space, submandibular space, and submental space), masticator space/secondary mandibular spaces (consisting of the masseteric space, pterygomandibular space, and temporal space), parapharyngeal space, primary maxillary space (consisting of the canine space, buccal space, infratemporal space), and cervical or deep neck spaces (consisting of the lateral pharyngeal space, retropharyngeal space, prevertebral space). [122, 129, 132, 134]
Primary maxillary space invovement can lead to orbital cellulitis or cavernous sinus thrombosis. An acute and toxic cellulitis (bacterial skin infection) of the primary mandibular spaces is known as Ludwig's angina. Extension of infection from the primary maxillary and primary mandible spaces can extend into the cervical or deep neck spaces which can lead to descending mediastinitis and airway obstruction. These conditions have been described above. [132, 134, 135]
52. Failure of Sedation/Anesthesia
It is possible for anesthesia and sedation provided during the surgery to remove a wisdom tooth to fail, causing the procedure to be cancelled, and needing to be rescheduled to be completed. Local anesthesia could fail if too long of a needle is used which could potentially cause the anesthetic to not be injected into the intended nerve. [140] There are several reasons for deep sedation/general anesthesia failure which includes increased levels of agitation and combativeness by the patient, parsoxysmal ventricular contractions occuring during the sedation, parsoxysmal ventricular contractions with desaturation, and blood pressure rising beyond a safe level to carry out the procedure. [73]
A 24 year old female with a history of mild anemia and hypothyroidism had her wisdom teeth removal cancelled after 20 minutes into the procedure because she became agitated and combative. She was given 200 mcg of Fentanyl, 5 mg of Midazolam, and 120 mg of a 2% lidocaine with 1:100,000 epinephrine. It is known that drugs known as benzodiazepines such as the Midazolam given, can cause pardoxical reactions which includes combativeness. [73]
In another case, a 25 year old female had her third molar surgery cancelled after 30 minutes as she developed premature ventricular contractions. She was given 100 mcg Fentanyl, 4 mg Midazolam, 40 mg Methohexitone, and 120 mg of a 2% lidocaine with 1:100,000 epinephrine. Epinephrine (also known as adrenaline) which was present in the local anesthesia is also released by the body during stress and pain. It can cause increased mean arterial pressure, tachychardia, increased systemic vascular resistence, increased cardiac output, and cardiac arrhythmias which are most commonly seen as premature ventricular contractions (PVCs). Methohexitone is also known to cause tachychardia which is when the heart beats too fast. Stress and anxiety can also lead to PVCs. [73]
53. Soft Tissue Damage (Lacerations, Abrasions, Contusions, and Burns)
It is possible that soft tissue can be damaged and lead to lacerations, abrasions, and contusions by the improper use of dental instruments by the person performing the surgery such as by their rough handing of a tissue retractor, their slide of a surgical drill, and them not being careful when using elevators, scalpels, sutures, and forceps scissors causing them to puncture or tear into soft tissue. An abrasion of the lips can be due to contact with a roating shank of a surgical drill (bur). An ointment or cream such as Vaseline should be applied to the lips if an abrasion occurs. The tearing of the mucosal flap and gingiva can also occur. [76, 77, 82, 122]
Soft tissue burns can be caused when a surgical drill starts to run hot due to the result of improper maintenance of the drill such as a dull bur or clogged or worn bearings or gears. A worn or clogged surgical drill will run hot due to a increase in power to the handpiece head or attachment in order to maintain handpiece peformance. Electrically induced heat known as diathermy which is used when performing electrocauterization to stop the bleeding from small blood vessels, can without proper care burn surrounding soft tissues as well. [76, 77, 78, 79]
The FDA (U.S. Food and Drug Administration) issued a public health notification directed at dental health professionals in December, 2007, regarding patient burns from electric dental handpieces. The notification stated some patients have had third degree burns occur which has required them to have plastic surgery. The FDA recommends that electric dental handpieces are properly maintained, encourages the training of personnel to ensure this occurs, suggests a method for tracking maintenance and service is used, and warns against the use of worn drills, burs, and poorly maintained electrical dental handpieces. The FDA issued another notice in September 2010, to worn dental profesionals about burns from electrical dental handpieces due to receiving numerous additional reports of patients being burned by electric dental handpieces since the original notice. [78, 79]
While not in the FDA's notice, it is important to know that any surgical instrument receiving sterlization should be allowed sufficient time to cool to prevent burns. [80, 81]
A 20 year old healthy male was administered a right inferior alveolar nerve block by a dental surgeon while having his wisdom teeth removed. During the procedure, the dental surgeon asked the dental assistant for a smaller straight elevator than the one that was currently in the extraction tray. The dental assistant gave the surgeon an elevator which he had asked for that had been recently sterilized. The surgeon applied it to the man's mouth without checking the tempearature. The surgeon noticed that the elevator was running hot when he touched the man's intraoral tissue which caused a first degree burn. Three days after the surgery, the man reported having pain of a 9 on a scale of 1 to 10 with 10 being the most severe. One week following the surgery the man saw a plastic surgeon. [80]

In another case a woman sustained a third degree burn to her face while she was under anaesthesia and having her wisdom teeth removed. The surgeon said that during surgery a defective bur guard in the drill overheated and slipped out of place and caused the drill to brush against the woman's lip. The burn caused a permanent scar below the right corner of her lips. [116]
In another case a woman sustained a severe second or third degree burn and/or laceration to her lower lip with a loss of feeling to her lower lip while having her wisdom teeth removed. During the surgery, which two dentists performed, the drill was vibrating violenty, was hot as it had overheated, and rested on her lip. It's not entirely clear if the drill was defectively designed or if the drill or bur guard caused the injury she sustained. [139]
54. Hearing Loss
A few people have suffered from hearing loss after a dental procedure. It is known that a tooth extraction can release microemboli into the circulation (small blood clots in the bloodstream). Hyperextension and extreme rotation of the cervical spine can cause stretching, shearing, or crushing of the vertebral artery which can result in intra-luminal thrombus formation and decreased blood flow (hypoperfusion). Microemboli released into the circulation can cause blood supply restriction (ischaemia) and obstruction of the blood supply (infarction) of the auditory portion of the inner ear (cochlea). [124, 125, 136]
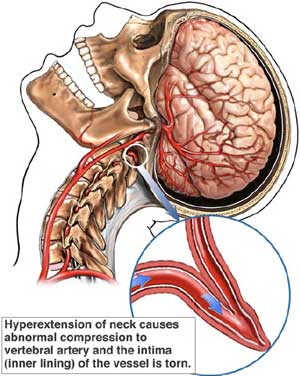
In one case a 18 year old woman had all 4 wisdom teeth extracted. After the surgery she had edema (swelling) and complained of hearing loss. She had an auditory experiment performed roughly 1 month before surgery. She had repeat auditory experiments performed after the extractions. Roughly 6 weeks after surgery her edema was gone and she repeated not being aware of any hearing loss. However, she had numerous audiograms over the next 19 months to assess her hearing. The low-frequency range of sound she was able to hear returned to normal which left her with the false impression that she had no hearing problem. In actuality she had mid-frequency hearing loss (around 2000 Hz) which "produced functional handicaps that are subtle and essentially unnoticeable..." She suffered bilateral hearing loss (both sides) and thus microemboli is likely not the source of her hearing loss. The exact cause of her hearing loss was impossible to determine so it was termed "idiopathic'' bilateral sensorineural hearing loss. [136]
55. Benign Paroxysmal Positional Vertigo (BPPV)
Benign paroxysmal positional vertigo can occur after wisdom teeth removal where one experiences symptoms of dizziness and vertigo. The dizziness is generally thought to be due to debris called otoconia which are small crystals of calcium carbonate that have dislodged from their hair cells and floated to abnormal positions. This can occur when the head is positioned in abnormal positions for a prolonged period of time. This can also be caused by bone drilling, osteotomes (which are instruments used with bone), and surgical hammers which can transmit percussive forces which can detach otoliths from the octoconial layer. The likely cause of BPPV during wisdom teeth extractions is by indirect trauma by the use of rotating tools or hammer and scalpel and the vibrations they cause which can damage semicircular canals and dissolve otoliths. Treatment includes the Epley maneuver or the Semont maneuver. [16, 17, 56, 137]
A 28 year old woman had four impacted wisdom teeth removed while under general anaesthesia. Immediately after recovery from the aneasthesia she developed intense vertigo with nausea whenever she turned her head to the left. She underwent Semont's liberatory manoeuvres for treatment. [56] Multiple other patients which have sent emails to this website's owner have described strange feelings inside their head along with dizziness and vertigo. One such patient complained of these symptoms continuing to persist to this day which is over 12 years since the extractions.
56. Wound Dehiscence / Poor Wound Healing
Wound dehiscence refers to a wound that has reopened after surgery or there is some disturbance with the healing process. It can be caused by general factors such as blood diseases and diabetes or local factors such as infection, dry socket, damage caused by dental instruments, reopening of sutures (stiches), and benign and malignant neoplasms (tumors). [122]
57. Herpes Zoster Syndrome (Shingles)
Wisdom teeth removal can potentially cause the reactivation of herpes zoster in the geniculate ganglion. This can lead to a cranial nerve motor neuropathy known as peripheral facial palsy which typically lasts until the anesthesia wears off but there can be a delay in the onset of symptoms. This can occur in people who have had chickenpox. Antiviral treatment is needed and this may be initially misdiagnosed as Bell's palsy. [12, 25]
58. Sepsis
While sepsis has been mentioned above in combination with another complication, it is also possible to develop sepsis by having wisdom teeth extracted. This can lead to a temperature of 105 degrees Fahrenheit, an extended hospital stay, and additional surgery. See the post https://blog.teethremoval.com/sepsis-after-wisdom-teeth-removal/ for additional details of a case.
59. Acquired Infection
There is potential for disease transmission through anything contaminated with fluids and tissues such as dental instruments, dental chairs, dental bib clips, and door knobs. [169] There is also potential for disease transmission when a patient who had their wisdom tooth or teeth removed repositions/touches a gauze pad put into their mouth postoperatively to stop bleeding if they had previously touched something in the dental office that was contaminated. Blood-borne diseases such as hepatitis B, C, D, or E, human immunodeficiency virus (HIV), spongiform encephalopathy, or syphilis can potentially be acquired. It is recommended that patients who have a blood-borne disease schedule any wisdom tooth extraction late in the day right before the office closes for the day to avoid spreading their infection to others. [63, 99] Clear instructions should be provided to patients regarding disposal of gauze sponges, spitting, and hand washing to prevent contamination of the dental office and potential spread of an acquired infection to others. [115]
It is also possible for syringes and needles to be re-used for multiple patients during intravenous sedation. A small amount of blood can remain in syringes and needles after an injection and this causes a risk of a spread of bloodborne viruses. In one case an oral surgeon in Colorado followed unsafe injection practices for nearly 12 years. [165, 166]
In one case that did not involve wisdom teeth but instead second molars, in Oklahoma dental assistants were found to be routinely administering sedation at an oral surgeon's office and lax sterilization procedures were being followed. One patient was tested positive for HIV and hepatistis C. [168] See the post https://blog.teethremoval.com/acquiring-hepatitis-c-at-the-oral-surgery-office/ for additional details.
While certainly very rare a 16 year old girl did receive a transfusion of tainted blood containing HIV while having her wisdom teeth removed. She then died six years later at 22 years of age. [13]
An man around 17 years old at the time received a transfusion of tainted blood containing HIV in 1983, while having his wisdom teeth removed. He had no symptoms until 1991 when a test showed he had AIDS. He later died at age 28 although he was born with hemophilia which is an inherited blood disorder. [14]
A woman claims to have acquired HIV from her dentist in December 1987, while having two wisdom teeth removed at the age of 19. She had no symptoms until March 1989, and was diagnosed with AIDS in January 1990. She later died at age 23. You can read more about this on Wikipedia http://en.wikipedia.org/wiki/Kimberly_Bergalis although the validity of this is questionable.
60. Death
Multiple people have died as a direct result of having their wisdom teeth removed. Learn about death occuring after wisdom teeth removal.
You may also be interested in learning about other dental deaths which do not include any of the deaths included on the deaths from wisdom teeth removal page.
Of Note (Sexual Assault)
Although not truly a complication from wisdom teeth removal (but still a potential risk of harm), numerous women at different time periods have accused their oral surgeon or dentist or a dental assistant of sexual assault while having their wisdom teeth extracted. Please read sexual assault under anesthesia for wisdom teeth removal for more information.
Other...
While this list is tries to be near exhaustive, the fact is is that a lot of things can go wrong. If you look carefully at both the death and dental malpractice pages of teethremoval.com (and associated references in the literature) you will find descriptions of a few other potential complications that can occur that were not explicity mentioned above. [42, 120] If efforts have to be made to resuscitate and restore consciousness during surgery other bodily injuries could potentially occur. Injury to your vocal cords and voice could potentially occur. [97]
A 20 year old woman had wisdom teeth removed and upon awakening from the surgery she stated she could not breathe. She was transferred to a local hospital and was discharged the following morning. The oral surgeon suspected she had an anxiety attack. [106]
A woman had two impacted wisdom teeth extracted along with two root canals filled by an oral surgeon and woke up from the surgery with a broken nose and deviated septum. She also developed a sinus infection which caused headaches and discharge down her throat containing pus. This was likely the result of being intubated with a No. 7 cuffed endotracheal tube by the anesthesiologist. [148]
A woman had wisdom teeth removed by a dentist and she went home and slept. She awoke the next day with a sharp pain in her shoulder which was later diagnosed as a long thoracic nerve injury. [152]
In addition, if you are pregnant a miscarriage could potentially occur. A woman had two wisdom teeth extracted during her third trimester of pregnancy in which only a local anesthetic was used. Three to five days later the fetus was determined to be dead. [150]
In a case in 1982 in Canada a man had his left parotid duct severed which led to infection around his left ear while having wisdom teeth removed. He later had a parotidectomy which caused damage in the "hinge" to his jaw and deafness in one ear along with left facial paralysis. [162]
In a shocking case in New Zealand a healthy young man was scheduled to have a wisdom tooth removed and woke up with a scar on his inner thigh and unable to move his leg. The surgeon had misspelt 'lower left wisdom tooth' as 'adductor longus tendon' and was described as "... a mistake anyone could have made." He was given $100,000. [158]
Other Unfortunate Occurrences - Being Told Condition / Symptoms Not Related to Surgery
Unforuntately there is a risk that you may be told after surgery that a complication or symptoms you experience after surgery is not related to the surgery to extract your wisdom teeth. This poses a problem and one should notify others where they live that they are having surgery and potentially have a backup oral surgeon or dentist to visit in case this were to occur. However, if you don't have a backup dentist you can always quickly find a dentist fast from a site like emergencydentist247.com or look through local results in Google. Remember that in the U.S. medicine and dentistry is a for profit business and the oral surgeon and/or dentist may be trying to protect themselves from a potential malpractice suit.
In one case a 23 year old healthy woman in 1975, in Illinois, had four wisdom teeth removed by an oral surgeon. She later developed pain and swelling in her right jaw which later become very stiff and barely able to move. She later called the oral surgeon's office and the doctor's nurse asked her if she was having pain in the area of the extraction to which she said no and then the nurse said the problems were not related to the oral surgery and to see a medical doctor. She then saw her family doctor who told her to see the oral surgeon. She then told him that the oral surgeon had refused to treat her. The family doctor then give a steroid medication and penicillin. The swelling and pain persisted and she called the oral surgeon's office who again told her to see the family doctor. She was later admitted to a hospital and had swelling, headaches, increased temperature, restricted jaw movement, and drainage from the right side of her mouth. She was given intravenous penicillin for 8 days and discharged from the hopsital 16 days later. Two weeks later she was rehospitalized with a temperature, facial swelling on her right side, a continuing abscess at the site of her wisdom tooth extraction. This time she remained in the hospital for 4 weeks and she was diagnosed with osteomyelitis. [146]
In another case a woman had four wisdom teeth extracted by an oral surgeon in Connecticut. After the surgery she contacted the surgeon's office and complained of a rash on the outside of her left check and was told over the phone that the "..condition was not related to the surgery." She filed a lawsuit and had an opinion letter from a plastic surgeon which said "I have significant oral surgery experience with third molar extraction. Thermal injuries to tissue can occur where electro cautery is excessive, ground is inadequate, or retraction with pressure is excessive.... Excessive pressure on the skin can result in necrosis of tissue and must be protected against. It is my opinion that the necrosis/scar on [her] left cheek was the result of either pressure or thermal injury that occurred during her wisdom tooth surgery." The plastic surgeon was not legally allowed to provide an opinion on the conduct of an oral surgeon and since the oral surgeon never saw the woman after surgery the lawsuit was dismissed (thrown out). [145]
You may be interested to learn the risks of deciding to keep your impacted wisdom teeth.
Updated November 30, 2019
References
1. Removing Wisdom Teeth. Best Treatments: clinical evidence for patients from the BMJ. Written September 2006.
2. Michael B. Lee, D.D.S. Patient's Guide to Wisdom Teeth. Cincinnati Oral Sugery. Accessed July, 2008.
3. J.M. Davies and Linda Campbell. Fatal Air Embolism During Dental Implant Surgery: A Report of Three Cases. Canadian Journal of Anaesthesia. January 1990. 37. 1. pages 112-121.
4. American Association of Oral and Maxillofacial Surgeons. White Paper on Third Molar Data.
Written March 2007.
5. The International Headache Society. The International Classification of Headache Disorders, 2nd edition. Written 2004.
6. Andy Kofke. Professor of Neuro-Anesthesiology and Critical Care at the University of Pennslvania. Brain Damage From Anesthetics.Written July 2007.
http://mkeamy.typepad.com/anesthesiacaucus/2007/07/brain-damage-fr.html
7. Michal Barak, MD and Yeshayahu Katz, MD, DSc. Chest. Microbubbles: Pathophysiology and Clinical Implications. October 2005. vol. 128. no. 4. pages 2918-2932.
8. Hassan G. Moghadam and Marco F. Caminiti. J Can Dent Assoc. Life-Threatening Hemorrhage after Extraction of Third Molars: Case Report and Management Protocol. 2002 68 (11) 670-4
http://www.cda-adc.ca/jcda/vol-68/issue-11/670.pdf
9. Dr. George Sándor. J Can Dent Assoc. Ontario Girl Suffers Septic Shock After Third Molar Removal. April 29, 2010. 75 a15. http://www.jcda.ca/article/a15
10. Jonathan B. Albilia and et. al. J Can Dent Assoc. Lemierre Syndrome from an Odontogenic Source: A Review for Dentists. May 17, 2010; 76 a47. http://www.jcda.ca/article/a47/
11. Herman Van Straalen and et. al. Chest. Mediastinitis with Fistula Formation to the Left Main Bronchus. 1994. 106. pages 623-624.
12. P.L. Ramchandani and et. al. British Journal of Oral and Maxillofacial Surgery. Subdural empyema and herpes zoster syndrome (Hunt syndrome) complicating removal of third molars. 2004. 42. pages 55-57.
13. Catherine Dunphy. Toronto Star. Quilt commemorates Canadians who died from AIDS. April 14, 1989. F3.
14. Abby Goodnough. The New York Times. The Neediest Cases; A Mother Remembers Her Son While Helping Others. January 8, 1995.
15. L.K. Cheung and et. al. Int. J. Oral Maxillofac. Surg. Incidence of Neurosensory Deficits and Recovery After Lower Third Molar Surgery: A Prospective Clinical Study of 4338 cases.
2010. vol. 39. issue 4. pages 320326.
16. Timothy C. Hain. Benign Paroxysmal Positional Vertigo. http://www.dizziness-and-balance.com/disorders/bppv/bppv.html July 19, 2010
17. Brauer HU. Quintessence International. Unusual Complications Associated with Third Molar Surgery: A Systematic Review. 2009. July-Aug. vol. 40. issue 7. pages 565-562.
18. Burgess B J. Emergency Casebooks. Epidural Abscess After Dental Extraction. page 231.http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1725590/pdf/v018p00231.pdf
19. Shyr-Chyr Chen and et. al. The American Journal of Emergency Medicine. Subcutaneous Emphysema and Pneumomediastinum After Dental Extraction. 1999. vol. 17 issue 7. pages 678-680.
20. Masato Funayama and et. al. The American Journal of Forensic Medicine and Pathology. Asphyxial Death Caused by Postextraction Hematoma. 1994. vol 15. issue 1. pages 87-90.
21. Jung-Chang Kung and et. al. Kaohsiung J Med Sci. Extensive Subcutaneous Emphysema After Extraction of a Mandibular Third Molar: A Case Report. 2009. 25. pages 562 - 566.
22. Mario F. Munoz Guerra and et. al. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. Subperiosteal Abscess of the Orbit: An Unusual Complication of the Third Molar Surgery. 2006. 102. e9-e13.
23. Dimitrious G. Balatsouras and et. al. The Journal of Laryngology and Otology. Submasseteric Abscess. January 2001. Vol. 115. pages 68-70.
24. J. Gallagher and J. Marley. British Dental Journal. Infratemporal and submasseteric infection following extraction of non-infected maxillary third molar.
Vol. 194. no 6. March 22, 2003.
25. Mahssine Tazi and et. al. J Oral Maxillofacial Surg. Facial Palsy Following Dental Extraction: Report of 2 Cases. July 2003. vol. 61. issue 7. pages 840-844.
26. P. Revol and et. al. Rev Stomatol Chir Maxillofac. Brain abscess and diffuse cervico-facial cellulitis: complication after mandibular third molar extraction. October 2003. vol. 104. issue 5. pages 285-289.
27. Cassio Edvard Sverzut and et. al. Journal of Oral and Maxillofacial Surgery. Removal of a Maxillary Third Molar Accidentally Displace Into the Infratemporal Fossa via Intraoral Approach Under Local Anesthesia: Report of Case. Vol. 67. Issue 6. June 2009. Pages 1316-1320.
28.
Serhat Yalcin and et. al. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. Accidental Displacement of a High-Speed Handpiece Bur During Mandibular Third Molar Surgery: A Case Report. 2008. 105. e29-e31
29. J Sekine and et. al. Int J Oral Maxillofac Surg. Bilateral pneumothorax with extensive subcutaneous emphysema manifested during third molar surgery: A case report. Oct 2000. vol. 28. issue 5. pages 355-357.
30. M. Wen-Der Yun and et. al. European Archives of Oto-Rhino-Laryngology. Cavernous sinus thrombosis following odontogenic and cervicofacial infection. 1991. 248. pages 422-424.
31. David A. Albert. Ask the Dentist. June 18, 2008.
32. N. Shah and J. B. Bridgman. British Dental Journal. An extraction complicated by lateral and medial pterygoid tethering of a fractured maxillary tuberosity. vol. 198. no. 9 May 14, 2005.
33. Yitzhak Woldenberg and et. al. Med Oral Patol Oral Cir Bucal. Iatrogenic mandibular fracture associated with third molar removal. Can it be prevented? 2007. 12. e70-72.
34. Cai H-X and et. al. Dental Traumatology. Dislocation of an upper third molar into the maxillary sinus after a severe trauma: a case report. 2007. 23. pages 181-183.
35. Klara Sokler and et. al. Acta Stomat Croat. Treatment of Orantral Fistula. 2002. pages 135-140.
36. Topazian, Goldberg, and Hupp. Oral and Maxillofacial Infections. 4th Edition. 2002 W.B. Saunders Company.
37. Guillermo Gomez-Oliveira and et. al. Med Oral Patol Oral Cir Buccal. Delayed removal of a maxillary third molar from the infratemporal fossa. May 1, 2010. 15 (3) e509-11.
38. K. Gadhia and et. al. Int. J. Oral Maxillofac. Traumatic Pseuodlipoma: Herniation of Buccal Fat Pad, A Report of Two Cases. 2008. 38. pages 694-703.
39. Enrique Marco de Luca and et. al. Surg Oral Med Oral Pathol Oral Radiol Endod. Life-threatening pseudoaneuryms of the facial artery after dental extraction: successful treatment with emergen endovascular embolization. 2008. vol. 106. pages 129-132.
40. P. Ricalde and et. al. Int J. Oral Maxillofac. Surg. Paediatric necrotizing fasciitis complicating third molar extraction: report of a case. 2004. 33. pages 411-414.
41. Farshid Rayati and et. al. J Oral Maxillofac Surg. Facial Artery Pseudoaneurysm Following Surgical Removal of a Mandibular Molar. 2010. 68. pages 1683-1685.
42. Strauss H.R. and et. al. J Oral Surg. Ludwig angina, empyema, pulmonary infiltration, and pericarditis secondary to extraction of a tooth. March 1980. vol 38. issue 3. pages 223 - 239.
43. Didier D. Malis and et. al. J Oral Maxillofac Surg. Lemierre Syndrome and Descending Necrotizing Mediastinitis Following Dental Extraction. 2008. 66. pages 1720-1725.
44. Ney Medeiros and Gustavo Gaffree. J Oral Maxillofac Surg. Accidental Displacement of Inferior Third Molar into the Lateral Pharyngeal Space: Case Report. 2008. 66. pages 578 - 580.
45. Gary Warburton and Jaime S. Brahim. J Oral Maxillofac Surg. Intraorbital Hematoma After Removal of Upper Third Molar: A Case Report. 2006. 64. pages 700-704.
46. L. A. Palmersheim and M. K. Hamilton. Journal of Oral and Maxillofacial Surgery. Fatal cavernous sinus thrombosis secondary to third molar removal. 1982. vol 40. issue 6. pages 371-376.
47. E. Welsley Ely and et. al. The American Journal of Medicine. Thoracic complications of dental surgical procedures: Hazards of the dental drill. November 1993. vol. 95. issue 5. pages 456-465.
48. Russel A. Faust. PhD, MD. 8 Dangerous Complications of Sinusitus, But 3 That Can Kill. April 19, 2010.
49. Laurie Loevner and Jennifer Bradshaw. Paranasal Sinuses and Adjacent Spaces.
50. David L. Baker. D.D.S. Consent for Treatment. Valencia Oral and Maxillofacial Surgery.
51. H. Ryan Kazemi. DMD. The Wise Guide to Wisdom Teeth Extraction: Making Engaged Decisions about Your Wisdom Teeth Extraction. 2010.
52. Tooth extractions aftercare: Common post extraction instructions / dry sockets. http://www.animated-teeth.com/tooth_extractions/t7_instructions_post-op.htm Accessed October 19, 2010.
53. Heath Hendrickson. DDS.
54. American Association of Oral and Maxillofacial Surgeons. Third Molar Multidiscplinary Conference. October 19, 2010.
55. Raymond L. Wiggins and et. al. Myositis Ossificans Circumscripta of the Buccinator Muscle: First Report of a Rare Complication of Mandibular Third Molar Extraction. J Oral Maxillofac Surg. 2008. 66. pages 1959-1963.
56. Luca D'Ascanio and Fabrizio Salvinelli. Benign Paroxysmal Positional Vertigo: An Unusual Complication of Molar Teeth Extraction. Letters to the Editor/ British Journal of Oral and Maxillofacial Surgery. 2007. 45. pages 176 -177.
57. Bodner L, et al. Characteristics of iatrogenic mandibular fractures associated with tooth removal: a review and analysis of 189 cases. Br J Oral Maxillofac Surg. 2010.
58. Nikolaos Sakkas and et. al. Orbital abscess after extraction of a maxillary wisdom tooth. Br J Oral Maxillofac Surg. 2007. 45. pages 245-246.
59. Elgazzar, R. F. and et. al. Aspiration of an Impacted Lower Third Molar During its Surgical Removal Under Local Anaesthesia: A Case Report and Review of the Literature. Int. J. Oral Maxillofac. Surg. 2007. 36. pages 362-364.
60. Gregory A. Conner and Michael Duffy. Myositis Ossificans: A Case Report of Multiple Recurrences Following Third Molar Extractions and Review of the Literature. J Oral Maxillofac Surg. 2009. 67. pages 920-926.
61. Hao-Hueng Chang and et. al. Effectiveness of an educational program in reducing the incidence of wrong-site tooth extraction. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004. 98. pages 288-294.
62. Janice S. Lee and et. al. Prevention of Wrong-Site Tooth Extraction: Clinical Guidelines. J Oral Maxillofac Surg. 2007. 65. pages 1793-1799.
63. Maria Chatzoudi. Handling Post-Dental Extraction Patients: How to Avoid Trans-Infection of Blood-Borne Diseases. J Oral Maxillofac Surg. 2009. 67. pages 2583 - 2586.
64. David H. Perrott and et. al. Office-Based Ambulatory Anesthesia: Outcomes of Clinical Practice of Oral and Maxillofacial Surgeons. J Oral Maxillofac Surg. 2003. 61. pages 983-995.
65.
Stuart J. Spitalnic and Andrew Sucov. Ludwig's Angina" Case Report and Review. The Journal of Emergency Medicine. 1995. vol 13. no. 4. pages 499-503.
66. Kenneth J. Mack. M.D. PhD. New Daily Persistent Headache in Children and Adults. Current Pain and Headache Reports. 2009. 13. pages 47-51.
67. Kenneth J. Mack. M.D. PhD. What Incites New Daily Persistent Headache in Children? Pediatric Neurology. 2004. vol. 31. no. 2. pages 122-125.
68. Todd D. Rozen. Chapter 44: New daily persistent headache. Handbook of Clinical Neurology. vol. 97 (3rd series) Headache. 2011. Elsevier B.V.
69. M. Anthony Pogrel. Broken Local Anesthetic Needles: A Case Series of 16 Patients, With Recommendations. J Am Dent Assoc. 2009. 140. pages 1517-1522.
70. Melissa Nann. Dentist Not Negligent For Needle Breaking Off in Surgery Patient's Gums. The Legal Intelligencer. Philadelphia. Monday, December 1, 2003. page 1.
71. Marcello Augello and et. al. Needle breakage during local anesthesia in the oral cavity - a retrospective of the last 50 years with guidelines for treatment and prevention. Clin Oral Invest. Springer - Verlag. 2010.
72. Special Supplement to The Journal of the American Dental Association. Managing Emergencies: What dentists and staff need to know. JADA. vol 141. May 2010.
73. Figen Cizmeci Senel and et. al. Evaluation of Sedation Failure in the Outpatient Oral and Maxillofacial Surgery Clinic. J Oral Maxillofac Surg. 2007. 65. ages 645-650.
74. Thomas B. Dodson and Srinivas M. Susarla. Impacted Wisdom Teeth. Search date July 2009. Clinical Evidence. 2010. 04:1302. pages 1- 17.
75. Friedman JW. The prophylactic extraction of third molars: a public health hazard. Am J. Public Health. 2007. 97. pages 1554-1559.
76. International Medical College (IMC). Dentoalveolar surgery: intra-operative soft-tissue complications. Accessed December 15, 2010. http://www.med-college.hu/de/wiki/artikel.php?id=182&lan=2
77. John Doran. Soft Tissue Damage. Accessed May 21, 2010. http://www.exodontia.info/SoftTissueDamage.html
78. Daniel G. Schultz. M.D. FDA Public Health Notification: Patient Burns from Electric Dental Handpieces Issued December 12, 2007.
79. FDA. Safety Investigation of Patient Burns Associated with Electric Dental Handpieces and Electric Oral Bone-cutting Handpieces. September 23, 2010.
80. Yehuda Zadik. DMD. MHA. Iatrogenic Lip and Facial Burns Caused by an Overheated Surgical Instrument. CDA Journal. September, 2008. vol. 36. no. 9. pages 689 - 691.
81. William A. Rutala and et. al. Patient injury from flash-sterilized instruments. Infect. Control Hosp. Epidemiol. July 1999. 20. page 458.
82. Edward Ellis III, James R. Hupp, and Myron R. Tucker. Contemporary Oral and Maxillofacial Surgery. 4th edition. Mosby. December 5, 2002.
83. C. Katre and et. al. Inferior alveolar nerve damage caused by bone wax in third molar surgery. Int. J. Oral Maxillofac. Surg. 2010. 39. pages 511-513.
84. American Association of Oral and Maxillofacial Surgeons. Position Paper on Bisphosphonate-Related Osteonecrosis of the Jaw2009 Update.
85. Postextraction Problems. The Merck Manuals: The Merck Manual for Healthcare Professionals. Accessed December 16, 2010. http://www.merckmanuals.com/professional/sec08/ch096/ch096d.html?qt=post%20extraction%20problems&alt=sh
86. Osteogenesis Imperfecta Foundation. What is Osteonecrosis of the Jaw? Breatkthrough. Summer 2006.
87. Current Clinical Practice and Parameters of Care: The Management of Patients with Third Molar Teeth. Faculty of Dental Surgery. The Royal College of Surgeons of England. London. September 1997.
88. Osteoradionecrosis. Fred Hutchinson Cancer Research Center. MOST Survivor's Notebook.
89. Hee-Kyun Oh. and et. al. Risk of osteoradionecrosis after extraction of impacted third molars in irradiated head and neck cancer patients. J Oral Maxillofac Surg. 2004. 62. pages 139-144.
90. S. Nabil and N. Samman. Incidence and prevention of osteoradionecrosis after dental extraction in irradiated patients: a systematic review. Int. J. Oral Maxillofac. Surg. 2010.
91. Bruno Ramos Chrcanovic and Antonio Luis Neto Custodio. Considerations of mandibular angle fractures during and after surgery for removal of third molars: a review of the literature. Oral Maxillofac Surg. 2010. 14. pages 71-80.
92. John Doran. Lingual Plate Fracture. Accessed May 21, 2011. http://www.exodontia.info/FracturedLingualPlate.html
93. Kyle J. Gernhofer. DDS. Concrescence of a Maxillary Second and Third Molar. CDA Journal. July 2009. vol. 37. no. 7 pages 479-481.
94. Samprati J. Badjate and K.M. Cariappa. Concrescence. Report of a rare complication. NY State Dent J. January 2008 pages 56-57.
95. Masamichi Ono and et. al. A case of true concrescence diagnosed with cone-beam CT and in vico micro-CT. Oral Radiol. 2010. 26. pages 106-109.
96. Parameters of Care: Clinical Practice Guidelines for Oral and Maxillofacial Surgery. Anesthesia in Outpatient Facilities. AAOMS ParCare 07. 2007.
97. Alan E. Deegan. Anesthesia Morbidity and Mortality, 1988-1999: Claims Statistics From AAOMS National Insurance Company. Anesth Prog. 2001. 48. pages 89-92.
98. William G. Flick and et. al. Illinois Dental Anesthesia and Sedation Survey for 2006. Anesth Prog. 2007. 54. pages 52-58.
99. Takenobu Wada and et. al. Blood contamination of environmental surfaces in outpatient oral surgery operatory. Asian Journal of Oral and Maxillofacial Surgery. vol. 22. issue 1. pages 12-16. 2010.
100. Serhat Yalçın and et. al. Surgical Treatment of Oroantral Fistulas: A Clinical Study of 23 Cases. J Oral Maxillofac Surg. Vol. 69. Issue 2. pages 333-339. 2011.
101. Enrique Ferrús-Torres and et. al. Informed Consent in Oral Surgery: The Value of Written Information. J Oral Maxillofac Surg. Vol. 69. Issue 1. pages 54-54. 2011.
102. The Fort Scott Tribune. Peter Gott. M.D. Self-catheterization is risky. March 15, 2001. 10
103. KVBC. Surgeon Pulled Tooth Directly For Profit. https://blog.teethremoval.com/surgeon-pulled-teeth-directly-for-profit/
104. Anna. Dental malpractice leaving medicated gauze in for over a month.
Yahoo Answers. December 2010. http://answers.yahoo.com/question/index?qid=20101221181102AAQYZYx Accessed January 26, 2011.
105. S Kandasamy and DJ Rinchuse.
The wisdom behind third molar extractions. Australian Dental Journal. 54. pages 284-292. 2009. http://onlinelibrary.wiley.com/doi/10.1111/j.1834-7819.2009.01152.x/abstract
106. Lytle JJ, Stamper EP. 1988 Anesthesia survey of the Southern California Society of Oral and MaxillofaciaI Surgeons. J Oral MaxiIIofac Surg. vol. 47 pages 834-842. 1989.
107. Blondeau Francois and Nach G. Daniel. Extraction of impacted mandibular third molars: postoperative complications and their risk factors. J Can Dent Assoc. vol. 73. issue 4. 325. May 2007.
108. Lennart Hedström and Petteri Sjögren. Effect estimates and methodological quality of randomized controlled trials about prevention of alveolar osteitis following tooth extraction: a systematic review. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. vol. 103. issue 1. pages 8 - 15. 2007.
109. Daniel T. Richardson and Thomas B. Dodson. Risk of periodontal defects after third molar surgery: An exercise in evidence-based clinical decision making. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. vol. 100. no. 2. August 2005.
110. Y.Y Leung and L.K. Cheung. Risk factors of neurosensory deficits in lower third molar surgery: a literature review of prospective studies. Int. J. Oral Maxillofac. Surg. vol. 40. pages 1-10. 2011.
111. P. Soros, A. Frese, I.W. Husstedt and S. Evers. Cluster headache after dental extraction: implications for the pathogenesis of cluster headache? Cephalalgia. vol. 21. pages 619-622. 2001.
112. United Press International, Inc. Dental board chief pulled wrong teeth. May 26, 2009. http://www.upi.com/Top_News/2009/05/26/Dental-board-chief-pulled-wrong-teeth/UPI-86321243362366/
113. Takashi Yoshii and et al. Incidence of deep fascial space infection after surgical removal of the mandibular third molars. J Infect Chemother. vol. 7. pages 5557. 2001.
114. California Association of Oral and Maxillofacial Surgeons. The Compass. vol. XII. issue 3. page 21. Fall 2010.
115. Daniel M. Laskin. Improving the safety of the universal precautions. AAOMS Today. page 17. March/April 2011.
116. Kabalan v Hoghooghi. October 1, 2010. CA 09-02247. Supreme Court of the State of New York. Appellate Division, Fourth Judicial Department. http://www.nycourts.gov/courts/ad4/Clerk/Decisions/2010/10-01-10/all_decisions_10-01-10.pdf
117. Isabel Wilkerson. Indiana Law at Center Of Malpractice Debate. New York Times. August 20, 1990. http://www.nytimes.com/1990/08/20/us/indiana-law-at-center-of-malpractice-debate.html
118. Mark Burhenne DDS. How to Heal a Dry Socket. March 27, 2010. http://askthedentist.com/how-to-heal-a-dry-socket/ Accessed May 20, 2011.
119. Susanne Kinzer and et al. Severe deep neck space infections and mediastinitis of odontogenic origin: clinical relevance and implications for diagnosis and treatment. Acta Oto-Laryngologica. 129. pages 62-70. 2009.
120. L.G. Thijs and et al. Life threatening complications from a lower wisdom tooth. Int. J. Oral Maxillofac. Surg. vol. 11. issue 5. pages 310-315. 1982.
121. Enzo Porteri and et al. A strange chest pain after dental surgery. Intern Emerg Med. 3. pages 123-126. 2008.
122. Fragiskos D. Fragiskos DDS PhD. Oral Surgery. Springer-Verlag Berlin Heidelberg. 2007.
123. Amish Shah, Neeta Mehta, and Derek P Von Arx. Fracture of a Dental Needle during Administration of an Inferior Alveolar Nerve Block. Dental Update. 36. pages 20-25. 2009.
124. Roy W R Farell and et al. Sudden deafness after dental surgery. BMJ. 303. page 1034. 1991.
125. T. S. Tan and et al. Acute sensorineural hearing loss immediately following a local anaesthetic dental procedure. Eur Arch Otorhinolaryngol. 264. pages 99102. 2007.
126. M. Kotli and et al. Case report of a displaced wisdom tooth. Oral Surgery. 3. pages 40-42. 2010.
127. Amit Sethi. Root fragment in the ostium of the maxillary sinus. British Journal of Oral and Maxillofacial Surgery. 47. pages 572-573. 2009.
128. F. Chandrasena and et al. Removal of a root from the maxillary sinus using functional endoscopic sinus surgery. British Journal of Oral and Maxillofacial Surgery. 48. pages 558-559. 2010.
129. Martin Kunkel and et al. Severe Third Molar Complications Including DeathLessons from 100 Cases Requiring Hospitalization. J Oral Maxillofac Surg. 65. pages 1700-1706. 2007.
130. V. Patel and et al. Osteomyelitis presenting in two patients: a challenging disease to manage. British Dental Journal. vol. 29. no. 8. pages 393-396. 2010.
131. Ralf Schoen and et al. Osteomyeltis of the mandible following third molar surgery: A regrettable consequence in a healthy patient. Quintessence International. vol. 40. no. 5. pages 351-354. 2009.
132. John Doran. Cervico-Fascial Infections Ludwig's Angina. http://www.exodontia.info/Ludwigs_Angina.html Accessed May 22, 2011.
133. Jeffrey Buyten and Francis B. Quinn. Deep Neck Space Infections. October 5, 2005.
134. Nino Zaya MD. Diagnosis and Management of Odontogenic Infections. November 2, 2006.
135. Charles W. Cummings and et al. Cummings Otolaryngology: Head and Neck Surgery. 4th Edition. Mosby Inc. 2005.
136. Richard E. Wilson and et al. Bilateral Idiopathic Sensorineural Hearing Loss following Dental Surgery. J Am Acad Audiol. 20. pages 180186. 2009.
137. Giuseppe Chiarella and et al. Benign paroxysmal positional vertigo after dental surgery. Eur Arch Otorhinolaryngol. 265. pages 119122. 2008.
138. Pacheco v. Ames. No. 72554-3. Supreme Court of Washington. 2003.
139. Angele Vandermark v. Hartford Hospital et al. X07CV034027734S. Superior Court of Connecticut, Judicial District of Hartford, Complex Litigation Docket at Hartford. July 21, 2008.
140. Jay W. Friedman DDS, MPH. Complete Guide to Dental Health. 2002.
141. David J. Strickland v. Board of Supervisors of Louisiana State University. No. CA-0445. Court of Appeal of Louisiana, Fourth Circuit. May 16, 1983.
142. Donna Cavagnetto v James A Pierce. Case No. CA96-02-021. Court of Appeals of Ohio, Twelfth Appellate District, Clermont County. November 25, 1996.
143. Srinivas M. Susarla and et al. Third molar surgery and associated complications. Oral Maxillofacial Surg Clin N Am. 15. pages 177-186. 2003.
144. Danny Williams v. Warden Pat Hurley. Case No. 2:05cv1022. United States District Court for the Southern District of Ohio, Eastern Divison. April 23, 2007.
145. Leah Nestico v. Brett A. Weyman. HHDCV096003675. Superior Court of Connecticut, Judicial District of Hartford at Hartford. May 19, 2011.
146. Jean Ann Longman v Clement Jasiek. No. 80-94. Appellate Court of Illinois, Third District. December 19, 1980.
147. Margie Rosales v. James Loyola and St. Paul Fire & Marine Insurance Company. No. 2007-CA-0517. Court of Appeal of Louisiana, Fourth Circuit. December 12, 2007.
148. Gwynne Mccarthy v. Charles W. Hauck. Appeals Court of Massachussetts, Middlesex. April 5, 1983.
149. Harrison V. Pittman v. Linda Hodghes. No. 54,501. Supreme Court of Mississippi. December 19, 1984.
150. Dillard Rhodus v Paul D. Wheeler and Gary D. Hansen. WD 49584. Court of Appeals of Missouri. June 18, 1996.
151. Heather Sharp v Frank L. Weber. 2009-05121. Supreme Court of New York, Appellate Division, Second Department. October 19, 2010.
152. Angela L. Faris v. Harold F. Doench Jr. et al. C.A. Case No. 13933. Court of Appeals of Ohio, Second Appellate District, Montogomery County. March 2, 1994.
153. Snyder et al. v. Ash et al. No. CA-8211. Court of Appeals of Ohio, Fifth Appellate District, Stark County, March 11, 1991.
154. Marjorie Richardson v. Glenn L. Keiper et al. C.A. No. 12566. Court of Appeals of Ohio, Ninth Appellate District, Summit County. September 24, 1986.
155. Megan Rae Comstock v M. James Clark. No. 09-07-300 CV. Court of Appeals of Texas, Ninth District Beaumont, October 25, 2007.
156. Leonard Dolce and Charles Leonard Dolce v Kirsten Husak. No. 03-07-00125-CV. Court of Appeals of Texas, Third District, Austin. January 25, 2008.
157. Ray K. Oukrop v Dennis Wasserburger. No. 86-306. Supreme Court of Wyoming. June 1, 1998.
158. Joe Bennett. Waikato Times. National crisis fuels groin tensions. October 5, 2011. http://www.stuff.co.nz/waikato-times/opinion/5734613/National-crisis-fuels-groin-tensions
159. H. Kocaelli, H. A. Balcioglu, and T.L. Erdem. Displacement of a maxillary third molar into the buccal space: anatomical implications apropos of a case. Int. J. Oral Maxillofac. Surg. vol. 40. issue 6, pp 650-653. 2011.
160. M. Manfredi and et al. Bisphosphonate-related osteonecrosis of the jaws: a case series of 25 patients affected by osteoporosis. Int. J. Oral Maxillofac. vol 40. issue 3. pp 285-291. 2011.
161. J. Sedy and R. Foltan. The origin of traumatic neuroma development. Int. J. Oral Maxillofac. vol. 40. issue 1. pp. 125-126. 2011.
162. Edgar v. Freedman. 1997 B.C.J. No. 1643. British Columbia Court of Appeal. July 8, 1997.
163. Javier Montero and Giuseppe Mazzaglia. Effect of Removing an Impacted Mandibular Third Molar on the Periodontal Status of the Mandibular Second Molar. J. Oral Maxillofac. Surg. vol. 69. issue 11. pages 2691-2697. 2011.
164. Adam Weiss, Peter Nelson, Reza Movahed, Earal Clarkson, and Harry Dym. Necrotizing Fasciitis: Review of the Literature and Case Report. J. Oral Maxillofac. Surg. vol. 69. issue 11. pages 2786-2794. 2011.
165. Colorado Department of Public Health and Environment. Unsafe Injections at an Oral Surgeon's Offices. July 20, 2012.
166. Blair Shiff. 9News. Oral surgeon also investigated for Rx fraud. July 14, 2012. Accessed July 29, 2012.
167. M. Anthony Pogrel. What Are the Risks of Operative Intervention? J. Oral Maxillofac. Surg. vol. 70, pp. 30-36, 2012, suppl. 1.
168. Donna Domino, 7,000 patients warned of possible hepatitis, HIV exposure, DrBicuspid.com. March 29, 2013.
169. "Study: Dental Bib Clips Can Harbor Oral and Skin Bacteria Even After Disinfection," April 2, 2013. http://dentalbibclipbacteria.com/ Accessed April 6, 2013.
170. Majid Eshghpour, Naser Mohammadzadeh Rezaei, and AmirHossein Nejat, "Effect of Menstrual Cycle on Frequency of Alveolar Osteitis in Women Undergoing Surgical Removal of Mandibular Third Molar: A Single-Blind Randomized Clinical Trial," Journal of Oral and Maxillofacial Surgery, vol. 71, pp. 1484-1489, 2013.
171. Elena Queral-Gody, Eduard Valmaseda-Castellon, Leonardo Berini-Aytes, and Cosme Gay-Escoda, "Incidence and evolution of inferior alveolar nerve lesions following lower third molar extractions," Oral Surgery, Oral medicine, Oral Pathology, Oral Radiology and Endodontics, vol. 99 pp. 259-264, 2005
172. Wataru Kawashima, Katsuhiko Hatake, Yoshifumi Morimura, Risa Kudo, Mari Nakanishi, Shigehiro Tamaki, Shogo Kasuda, Katsuya Yuui, and Akiko Ishitani, "Asphyxial death related to postextraction hematoma in an elderly man," Foresnic Science International, vol. 288, e47-e49, 2013.
173. Giovanni Gerbino, Emanuele Zavattero, Mattia Berrone, and Sid Berrone, "Management of needle breakage using intraoperative navigation following inferior alveolar nerve block," J. Oral Maxillofac. Surg. vol. 71, pp. 1819-1824, 2013.
174. Doksa Lee, Syoichiro Ishi, and Noburu Yakushiji, "Displacement of maxillary third molar into the lateral pharyngeal space," J. Oral Maxillofac. Surg. vol. 71, pp. 1653-1657, 2013.
175. Hans Urlich Bauer and et al., "Complications During and After Surgical Removal of Third Molars," OralHealth. June 1, 2013.
176. Michael Wasson, Basavaraj Ghodke, and Jasjit K. Dillon. "Exsanguinatiing hemorrhage following third molar extraction:report of a case and discussion of materials and methods in selective embolization," J. Oral Maxillofac. Surg. vol. 70, pp. 2271-2275, 2012.
177. Parviz Goshtasby, Reza Miremadi, and Ronald Warwar,. "Retrobulbar hematoma after third molar extraction: case report and review," J. Oral Maxillofac. Surg. vol. 68, pp. 461-464, 2010.
178. American Association of Oral and Maxillofacial Surgeons. Medication-Related Osteonecrosis
of the Jaw2014 Update. 2014.
|